

Quick Answer
Most herniated discs improve without surgery. Spine literature consistently reports that 60–90% of symptomatic lumbar disc herniations resolve with conservative care over 6 to 12 weeks. Effective non-surgical options include structured physical therapy, anti-inflammatory medication, activity modification, and epidural steroid injections. Surgery becomes appropriate only when conservative treatment fails after an adequate trial, or when red-flag neurological symptoms appear. If you've been told you need disc surgery, getting an independent second opinion is a reasonable and often recommended step before scheduling an operation.
Key Takeaways
- 60–90% of herniated discs heal or significantly improve without surgery within 6–12 weeks, according to data cited by organizations including the World Federation of Neurosurgical Societies (WFNS).
- Physical therapy with specific directional exercises (like McKenzie method) is the single most supported non-surgical treatment for herniated disc recovery.
- NSAIDs (ibuprofen, naproxen) are first-line medications; oral steroids and nerve pain drugs (gabapentin, pregabalin) may help in the acute phase.
- Epidural steroid injections can provide meaningful short-term pain relief, buying time for natural healing.
- Red flags requiring urgent evaluation: progressive leg or arm weakness, loss of bladder or bowel control, saddle-area numbness (these suggest cauda equina syndrome, a surgical emergency).
- Cervical and lumbar herniations respond to similar conservative principles, but cervical herniations need closer neurological monitoring.
- Chiropractic care and acupuncture may help with pain but have weaker evidence than physical therapy.
- An independent second opinion before surgery is a sensible, cost-effective step, especially when the recommendation is based on imaging alone.
What Exactly Is a Herniated Disc and How Do I Know If I Have One?
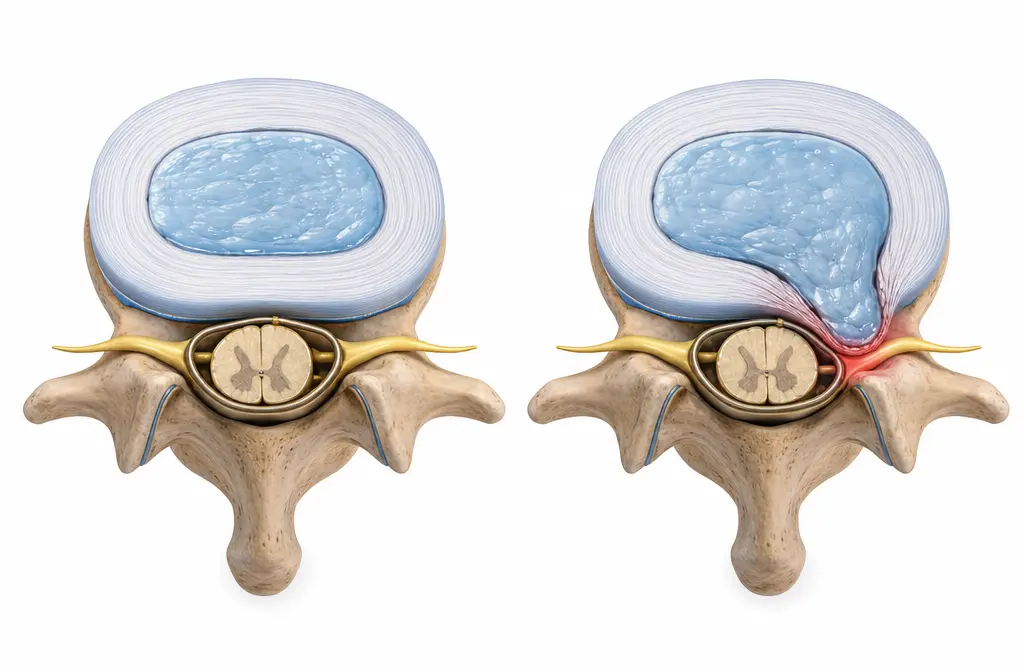
A herniated disc occurs when the soft, gel-like center (nucleus pulposus) of a spinal disc pushes through a tear in the tougher outer ring (annulus fibrosus) and presses on a nearby spinal nerve. This is different from a disc bulge, where the outer ring stretches but doesn't rupture.
Common symptoms include:
- Sharp, shooting pain down one leg (sciatica) for lumbar herniations, or down one arm for cervical herniations
- Numbness or tingling in the affected limb
- Muscle weakness in the leg or foot (lumbar) or hand and arm (cervical)
- Pain that worsens with sitting, bending, coughing, or sneezing
How it's diagnosed: A clinical exam by a doctor, combined with your symptom history, is usually enough to suspect a herniated disc. MRI is the gold-standard imaging test to confirm it. However, here's something many patients don't realize: MRI studies of people with zero back pain show that a significant percentage have disc herniations on imaging. This means an MRI finding alone does not necessarily explain your pain. Symptoms and clinical findings must match the imaging.
Common mistake: Assuming that a large herniation on MRI automatically means surgery. Disc size on imaging does not reliably predict who will need an operation. In fact, larger herniations sometimes resorb more completely than smaller ones.
How Long Does It Take to Heal a Herniated Disc Without Surgery?
Most people experience significant improvement within 6 to 12 weeks of conservative treatment. The body has a natural ability to resorb herniated disc material over time, and the inflammatory response that initially causes pain gradually subsides.
Realistic timeline:
Important context: "Healing" doesn't always mean the disc returns to its original shape on MRI. Many people become completely pain-free while the disc still looks abnormal on imaging. What matters is symptom resolution and functional recovery, not what the MRI shows.
Choose patience if: Your pain is improving week over week, even slowly. A gradual downward trend in symptoms is the best sign that conservative care is working.
Can a Herniated Disc Heal Completely Without Medical Intervention?
Yes, some herniated discs do heal without any formal medical treatment. The body's immune system treats extruded disc material as foreign tissue and gradually breaks it down through a process called resorption. Studies using serial MRI scans have shown that herniated disc fragments can shrink or disappear entirely over several months.
That said, "no medical intervention" doesn't mean "do nothing." Even without seeing a doctor, most people instinctively modify their activities, rest when needed, and take over-the-counter pain relievers. These are all forms of conservative treatment.
When self-care alone is reasonable:
- Mild to moderate pain without significant weakness
- Symptoms that are clearly improving over 2–4 weeks
- No bladder, bowel, or significant neurological changes
When you should seek professional guidance: If pain is severe, isn't improving after 2–3 weeks, or is accompanied by any neurological symptoms (weakness, numbness, changes in reflexes), professional evaluation is important. Early physical therapy guidance also tends to produce better outcomes than unguided self-care.
What Are the Best Exercises to Help a Herniated Disc Recover?
Specific directional exercises, particularly extension-based movements for lumbar herniations, are among the most effective non-surgical treatments available. The McKenzie Method (Mechanical Diagnosis and Therapy) is the best-studied exercise approach for disc-related pain.

Evidence-based exercises for lumbar herniated discs:
- Prone lying — Simply lying face-down for 5–10 minutes to gently encourage extension
- Prone press-ups (cobra) — Pressing the upper body up while keeping hips on the floor
- Standing back extensions — Placing hands on the lower back and gently arching backward
- Walking — Low-impact and promotes blood flow to the disc area
- Core stabilization — Once acute pain subsides, gentle core strengthening (bird-dogs, dead bugs, modified planks) helps prevent recurrence
For cervical herniated discs:
- Cervical retraction exercises (chin tucks)
- Gentle neck extension
- Isometric neck strengthening (once pain allows)
Exercises to avoid during the acute phase:
- Loaded spinal flexion (sit-ups, toe touches, heavy deadlifts)
- High-impact activities (running, jumping)
- Prolonged sitting, which increases disc pressure
Decision rule: If an exercise makes your leg or arm pain worse (peripheralizes symptoms), stop it. If it brings pain closer to the spine and away from the limb (centralizes symptoms), that's generally a positive sign and you should continue under guidance.
Can Physical Therapy Really Fix a Herniated Disc?
Physical therapy is the most consistently recommended non-surgical treatment for herniated discs across international spine guidelines. It doesn't "fix" the disc in the sense of pushing it back into place, but it creates the conditions for natural healing while restoring function and reducing pain.
What a good physical therapy program includes:
- Assessment of movement patterns to identify which directions relieve or worsen symptoms
- Directional preference exercises (usually extension for lumbar discs)
- Manual therapy (joint mobilization, soft tissue work) for short-term pain relief
- Progressive loading as symptoms improve
- Education about the condition, prognosis, and self-management
How many sessions? Most clinical guidelines suggest 6–12 sessions over 6–8 weeks as an initial course. Many patients notice meaningful improvement within the first 2–4 weeks.
Common mistake: Stopping physical therapy too early because the pain decreases. The strengthening and stabilization phase that follows initial pain relief is what prevents recurrence. Patients who complete a full course of therapy have lower rates of re-injury.
Choose physical therapy first if: You have a new or recent herniated disc with radicular pain (sciatica or arm pain) but no red-flag symptoms. It's the safest, most cost-effective starting point.
What Pain Medications Help Most With Herniated Disc Symptoms?
First-line medication for herniated disc pain is a non-steroidal anti-inflammatory drug (NSAID) like ibuprofen or naproxen. These reduce both pain and the inflammation around the compressed nerve.
Medication options, ranked by typical use:
Important: Medication alone is not a treatment plan. It's a bridge that reduces pain enough for you to participate in physical therapy and stay active. The combination of medication plus structured exercise produces better outcomes than either alone.
Are Epidural Steroid Injections Effective for Herniated Disc Pain?
Epidural steroid injections (ESIs) deliver anti-inflammatory medication directly to the area around the compressed nerve. They can provide meaningful short-term pain relief (weeks to months) for many patients, which allows participation in physical therapy during the critical healing window.
When ESIs make the most sense:
- Pain is too severe to participate in physical therapy
- Oral medications aren't providing adequate relief
- You want to avoid or delay surgery
Limitations: ESIs treat symptoms, not the underlying herniation. They don't change the long-term outcome for most patients, but they can significantly improve quality of life during the acute phase. Most guidelines recommend a maximum of 3 injections per year.
Edge case: Some patients get excellent, lasting relief from a single injection. Others get minimal benefit. There's no reliable way to predict who will respond well, so a trial injection is often reasonable before considering surgery.
Are Chiropractors or Acupuncture Effective for Herniated Disc Pain?
Chiropractic spinal manipulation and acupuncture both have some evidence for general back pain relief, but the evidence specifically for herniated disc with radiculopathy is weaker than for physical therapy.
Chiropractic care:
- Low-force techniques (flexion-distraction) may help some patients with lumbar disc herniations
- High-velocity spinal manipulation should be approached cautiously with acute disc herniations, particularly in the cervical spine
- Best used as a complement to, not a replacement for, structured exercise
Acupuncture:
- May provide short-term pain relief through endorphin release and local anti-inflammatory effects
- Several international guidelines list it as a reasonable adjunct for chronic back pain
- Less evidence for acute radiculopathy specifically
Decision rule: If you want to try chiropractic care or acupuncture, use them alongside (not instead of) an active exercise program. If your symptoms aren't improving after 4–6 sessions, the treatment likely isn't working for you.
Which Treatments Work Best for Lumbar vs. Cervical Herniated Discs?
The core principles of herniated disc treatment without surgery apply to both lumbar and cervical herniations, but there are important differences.
Lumbar herniations (lower back):
- Extension-based exercises (McKenzie) are the primary movement approach
- Epidural steroid injections have the strongest evidence in the lumbar spine
- Walking is an excellent low-impact activity
- Most common location: L4-L5 and L5-S1
Cervical herniations (neck):
- Cervical retraction and gentle extension exercises
- Cervical traction (manual or mechanical) can help decompress the nerve
- Greater caution with manipulation therapies
- Closer monitoring for myelopathy (spinal cord compression), which is more common in the cervical spine
- Most common location: C5-C6 and C6-C7
Key difference: Cervical herniations that cause spinal cord compression (myelopathy) with symptoms like difficulty with fine motor tasks, gait changes, or bilateral hand numbness may need earlier surgical consideration than lumbar herniations.
How Much Does Non-Surgical Herniated Disc Treatment Cost?
Non-surgical treatment is substantially less expensive than surgery in virtually every healthcare system worldwide. Exact costs vary widely by country and insurance coverage, but the relative comparison is consistent.
Estimated cost ranges (these vary significantly by region):
- Physical therapy course (6–12 sessions): Typically a fraction of surgical costs
- Medications (NSAIDs, gabapentin): Generally inexpensive, especially generic versions
- Epidural steroid injection: Moderate cost; usually far less than surgery
- MRI scan: Varies widely but is a one-time diagnostic cost
- Microdiscectomy surgery (for comparison): Includes surgeon fees, anesthesia, facility costs, and post-operative rehabilitation
Beyond direct costs, non-surgical treatment usually means less time away from work and daily activities. Most people undergoing conservative care can continue modified work within days to weeks, while surgical recovery typically requires weeks of restricted activity.
Cost-saving tip: An online second opinion from an independent spine specialist before agreeing to surgery can be one of the most cost-effective steps you take. If the opinion confirms that conservative care is appropriate, you may avoid tens of thousands in surgical costs.
What Are the Risks of Leaving a Herniated Disc Untreated?
For most people, the risk of leaving a herniated disc to heal naturally is low. The majority of herniations improve on their own. However, there are specific situations where delayed treatment can cause lasting harm.
Low-risk scenarios (watchful waiting is appropriate):
- Pain without significant weakness
- Symptoms that are stable or improving
- Normal bladder and bowel function
Higher-risk scenarios (seek prompt evaluation):
- Progressive motor weakness — a foot drop that's getting worse, or grip strength that's declining
- Cauda equina syndrome (surgical emergency) — loss of bladder or bowel control, saddle-area numbness (inner thighs, perineum), bilateral leg symptoms
- Persistent severe pain beyond 6–12 weeks despite adequate conservative treatment
The real risk of "untreated" isn't usually permanent nerve damage from the disc itself. It's the secondary consequences: deconditioning from inactivity, chronic pain patterns that become harder to reverse, depression, and unnecessary disability. This is why structured conservative care (not just waiting) matters.
Who Should Avoid Non-Surgical Treatments for Herniated Discs?
Non-surgical treatment is not appropriate for everyone. Certain clinical presentations require urgent surgical evaluation, and delaying surgery in these cases can lead to permanent neurological damage.
Surgery should be considered urgently if you have:
- Cauda equina syndrome: Sudden bladder retention or incontinence, bowel incontinence, saddle numbness. This is a medical emergency requiring surgery within 24–48 hours.
- Rapidly progressive neurological deficit: Worsening weakness over days (e.g., developing foot drop or inability to lift the foot)
- Severe, disabling pain that doesn't respond to any conservative measures after 6–12 weeks of adequate treatment
Surgery may be considered electively if:
- You've completed a full course of conservative treatment (minimum 6 weeks, ideally 12) without meaningful improvement
- Your quality of life remains significantly impaired
- Imaging findings correlate with your symptoms and clinical exam
Important nuance: Having a herniated disc and having surgery-worthy symptoms are two different things. Many people with herniations on MRI have no symptoms at all. Surgery should treat the patient, not the MRI.
Common Mistakes People Make When Trying to Treat a Herniated Disc at Home
Knowing what not to do is just as valuable as knowing the right approach. These are the errors I see most often.
- Complete bed rest for more than 1–2 days. Extended rest weakens muscles and slows recovery. Gentle movement is better.
- Repeatedly flexing the spine. Bending forward, doing sit-ups, or stretching by touching your toes can push disc material further into the nerve. Extension is usually the better direction for lumbar herniations.
- Ignoring progressive weakness. Pain is one thing; losing the ability to lift your foot or grip objects is a red flag that needs medical attention.
- Relying only on passive treatments. Massage, heat packs, and TENS units feel good but don't change the underlying problem. Active exercise is essential.
- Stopping activity once pain improves. The strengthening phase after pain resolution is what prevents recurrence. Many people re-herniate because they return to full activity without rebuilding core stability.
- Catastrophizing based on MRI results. A report describing a "large herniation" can be frightening, but it doesn't predict your outcome. Focus on your symptoms and function, not the imaging language.
- Rushing to surgery without trying conservative care. Unless red flags are present, a minimum 6-week trial of structured conservative treatment is recommended by virtually all spine guidelines worldwide.
When Should I Stop Trying Natural Treatments and Consider Surgery?
Consider surgery when conservative treatment has been given a fair trial and has failed, or when neurological red flags emerge. Specifically:
Clear indications to discuss surgery with your doctor:
- No meaningful improvement after 6–12 weeks of structured conservative care (not just "waiting it out," but active physical therapy, appropriate medication, and possibly injections)
- Progressive neurological deficit despite treatment
- Cauda equina symptoms (emergency — don't wait)
- Pain so severe it prevents basic daily functioning and isn't responding to any conservative measures
The most common surgical options:
- Microdiscectomy: Small incision, removal of the herniated fragment pressing on the nerve. High success rate (approximately 85–90% for leg pain relief). Usually outpatient or one-night stay.
- Endoscopic discectomy: Even less invasive, using a small camera. Similar outcomes to microdiscectomy in experienced hands.
Before you schedule surgery, consider an independent second opinion. This is especially valuable if:
- Your surgeon recommended surgery based primarily on imaging without a thorough clinical correlation
- You haven't been offered or completed a structured conservative treatment program
- You have doubts about whether surgery is truly necessary
An online second opinion from an independent spine specialist can be obtained quickly and affordably. You send your imaging and medical records, and a specialist reviews your case without the potential bias of being the surgeon who would perform the procedure. Many patients who seek second opinions learn that conservative care is still a viable option.
Frequently Asked Questions
Q: Can I work with a herniated disc?
Most people can continue working with modifications during recovery. Avoid heavy lifting, prolonged sitting, and repetitive bending. Desk workers should take standing or walking breaks every 30–45 minutes. Discuss specific restrictions with your treating clinician.
Q: Is walking good for a herniated disc?
Yes. Walking is one of the best activities during herniated disc recovery. It promotes blood flow, gently loads the spine, and doesn't place excessive pressure on the disc. Start with short, comfortable distances and gradually increase.
Q: Should I use heat or ice for a herniated disc?
Ice may help in the first 48–72 hours to reduce inflammation. After that, many people find heat more soothing for muscle tension. Neither changes the disc itself, but both can provide temporary comfort. Use whichever feels better.
Q: Can a herniated disc come back after it heals?
Yes, recurrence is possible, particularly at the same spinal level. Completing a full physical therapy program including core strengthening significantly reduces recurrence risk. Maintaining a healthy weight and using proper lifting mechanics also help.
Q: How do I know if my sciatica is from a herniated disc or something else?
Sciatica (leg pain following the sciatic nerve path) is most commonly caused by a herniated disc, but spinal stenosis, piriformis syndrome, and other conditions can mimic it. An MRI combined with a thorough clinical exam is the best way to identify the cause.
Q: Is it worth getting a second opinion before disc surgery?
Absolutely. Spine surgery recommendations vary significantly between surgeons. Studies have shown that second opinions change the treatment plan in a meaningful percentage of cases. An independent review of your imaging and clinical history can confirm whether surgery is truly your best option or whether continued conservative care is reasonable.
Conclusion
Herniated disc treatment without surgery is not only possible for most people — it's the recommended first approach by spine specialists worldwide. The 60–90% spontaneous improvement rate means the odds are in your favor with structured conservative care.
Your action plan:
- Get an accurate diagnosis. Make sure your symptoms match your imaging findings.
- Start structured physical therapy with a therapist experienced in spinal conditions. Prioritize directional exercises and progressive strengthening.
- Use medication strategically — NSAIDs for inflammation, nerve pain drugs if needed, and consider an epidural injection if pain prevents participation in therapy.
- Stay active within your limits. Walk daily. Avoid prolonged bed rest and heavy spinal loading.
- Monitor for red flags. Progressive weakness, bladder or bowel changes, or saddle numbness require immediate medical attention.
- Give it time. Commit to at least 6–12 weeks of consistent conservative treatment before concluding it hasn't worked.
- Get a second opinion before surgery. If an operation is recommended, an independent review of your case — available online from qualified spine specialists — can confirm whether surgery is the right call or whether you have more conservative options to explore.
Your spine has a remarkable ability to heal. Give it the right support, the right time, and the right guidance, and surgery may never be necessary.