
Last updated: June 11, 2026
Quick Answer
A pinched nerve in the lower back happens when a spinal nerve root gets compressed or irritated, usually by a bulging disc, bone spur, or inflamed tissue. Most cases improve within 6 to 12 weeks with conservative care: movement, targeted exercise, and short-term pain relief. Surgery is rarely the first answer. Red flags such as loss of bladder or bowel control, saddle numbness, or progressive leg weakness require urgent medical attention.
Key Takeaways
- A pinched nerve in the lower back (lumbar radiculopathy) is most often caused by a herniated disc pressing on a nerve root.
- The hallmark symptom is pain, tingling, or weakness that travels down one leg, often called sciatica.
- Roughly 80 to 90 percent of cases settle without surgery within three months (NICE, Cochrane reviews).
- Movement helps; prolonged bed rest worsens recovery.
- True red flags (cauda equina symptoms) are rare but need emergency care.
- Imaging is not needed in the first 4 to 6 weeks unless red flags appear.
- An independent online second opinion is reasonable before agreeing to lumbar surgery.
What exactly is a pinched nerve in the lower back?
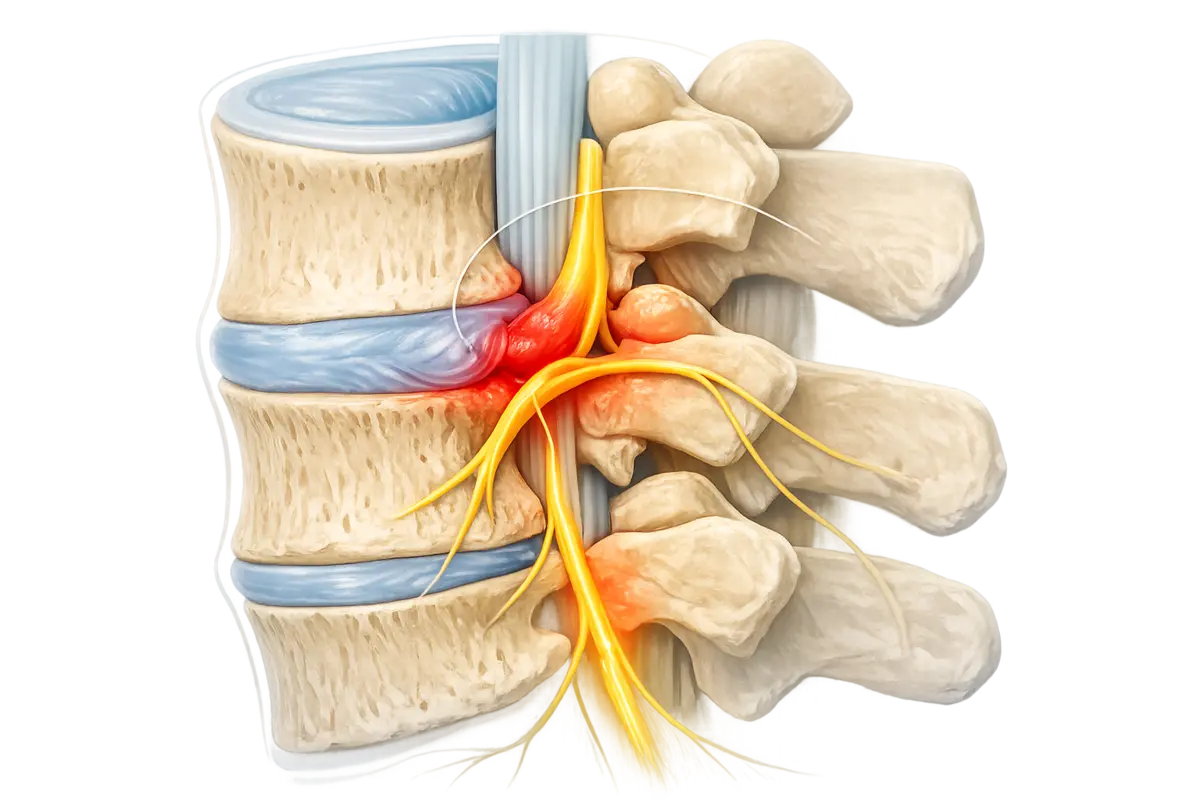
A pinched nerve in the lower back is mechanical or chemical irritation of a lumbar nerve root as it exits the spine. Clinicians call this lumbar radiculopathy. The compression usually occurs at the L4, L5, or S1 levels, which is why pain often radiates into the buttock, thigh, calf, or foot.
The nerve itself is not "trapped" in the everyday sense. It is irritated by:
- A herniated or bulging intervertebral disc
- Bone spurs from spinal osteoarthritis
- Thickened ligaments narrowing the spinal canal (spinal stenosis)
- Spondylolisthesis (one vertebra slipping forward)
- Less commonly, cysts, infections, or tumours
Inflammation around the nerve plays a bigger role than pure pressure. That's why anti-inflammatory strategies often work even when imaging still shows a disc bulge.
How do I know if I have a pinched nerve or just muscle pain?
The clearest distinguishing feature is leg symptoms. Muscle pain stays local. A pinched nerve sends signals along its path.
A simple at-home check: lie on your back and have someone slowly lift your straight leg. If pain shoots down the leg below 60 degrees, that suggests nerve root irritation. This isn't a diagnosis, but it's a useful clue.
Who is most likely to get a pinched nerve in their lower back?
Anyone can develop one, but risk rises with age, occupation, and lifestyle. People between 30 and 60 are most affected because discs are still hydrated enough to herniate (older discs tend to dry out and bulge differently).
Common risk factors:
- Heavy lifting with poor mechanics, especially with twisting
- Prolonged sitting (drivers, office workers)
- Smoking, which reduces disc nutrition
- Obesity and weak core musculature
- Pregnancy, due to ligament laxity and load shift
- Genetics: family history of disc disease
If you're in one of these groups and develop sudden leg pain after lifting something, a disc-related pinched nerve is a reasonable working assumption until proven otherwise.
Can a pinched nerve in the lower back heal on its own?
Yes, most do. Multiple Cochrane reviews and NICE guidance on low back pain and sciatica confirm that the majority of lumbar radiculopathy cases improve without surgery. The body reabsorbs disc material, inflammation settles, and the nerve recovers.
Typical natural history:
- Weeks 1 to 2: Worst pain, often sharp leg symptoms
- Weeks 3 to 6: Gradual easing, pain "centralises" toward the back
- Weeks 6 to 12: Most people functional again
- 3 to 6 months: Continued improvement; residual numbness may persist longer
About 10 to 20 percent of patients still have meaningful symptoms at 12 weeks. That's the group where escalation, including a discussion of injection therapy or surgery, becomes reasonable, and where a second opinion is most valuable.
What are the best exercises to help a pinched nerve?
Gentle, directional movement is the foundation. The goal is to reduce nerve tension, calm inflammation, and restore core support. Start slow, stay below sharp pain, and progress gradually.
A safe starting routine (general guidance, not personal medical advice):
- Pelvic tilts — Lie on your back, knees bent, gently flatten your lower back into the floor. 10 reps.
- Knee-to-chest stretch — One knee at a time, hold 20 seconds. Both sides.
- Cat-cow — On hands and knees, alternate arching and rounding. 10 slow cycles.
- Nerve glides (sciatic floss) — Seated, slowly extend one knee while tilting your head back, then reverse. 10 gentle reps.
- Glute bridges — Lift hips from the floor, hold 3 seconds. 10 reps.
- Walking — 10 to 20 minutes daily, increasing as tolerated.
What to avoid early on: heavy deadlifts, deep forward bends, sit-ups, and long sitting. If an exercise sends pain further down the leg, stop. If it eases leg pain (centralisation), that's a good sign.
What are common mistakes people make when treating a pinched nerve?
I see the same patterns repeatedly in second-opinion consultations.
- Bed rest beyond 1 to 2 days. Strong evidence shows this slows recovery.
- Chasing the perfect MRI. Imaging findings often don't match symptoms; many pain-free adults have disc bulges.
- Rushing into surgery before 6 to 12 weeks without red flags or progressive neurological loss.
- Stopping all activity instead of modifying it.
- Long-term opioid use. Not effective for nerve pain and carries dependency risk.
- Aggressive spinal manipulation during the acute, highly inflamed phase.
- Ignoring red flags because "it's just back pain."
The single biggest mistake I encounter is patients consenting to surgery without understanding that their condition statistically tends to improve on its own.
"An MRI shows anatomy, not pain. The decision to operate should rest on the clinical picture, not the scan alone."
Can a pinched nerve cause permanent damage if left untreated?
Permanent damage is uncommon but possible. The risk rises when severe compression continues for weeks to months without improvement, or when red-flag symptoms are missed.
Warning signs of potential nerve injury:
- Progressive weakness (a foot that's getting harder to lift)
- Numbness expanding rather than receding
- Loss of reflexes
- Cauda equina syndrome: saddle numbness, bladder or bowel dysfunction, sexual dysfunction — this is a surgical emergency, ideally treated within 24 to 48 hours
Mild residual numbness or tingling after recovery is common and usually not disabling. But weakness that worsens over weeks should always be evaluated promptly.
How long does it typically take to recover from a pinched nerve?
Most people see meaningful improvement within 6 to 12 weeks. Full recovery, including resolution of numbness, can take 3 to 6 months. A smaller group needs longer.
Rough timeline:
- Day 1 to 14: Acute phase. Manage pain, stay gently mobile.
- Week 2 to 6: Subacute. Begin structured physiotherapy.
- Week 6 to 12: Functional recovery. Return to most activities.
- 3 to 6 months: Residual symptoms continue to fade.
- Beyond 6 months: If still significantly impaired, formal reassessment is warranted.
Recovery is rarely linear. Flares are normal and don't mean you're back to square one.
Physical therapy vs chiropractic care: what's the difference?
Both can help, but they're structured differently. Physiotherapy focuses on active rehabilitation: exercise, motor control, education, and graded return to activity. Chiropractic care traditionally centres on manual spinal adjustments, though many modern chiropractors also include exercise.
For lumbar radiculopathy, international guidelines (NICE, WFNS) generally favour structured exercise-based rehabilitation as first-line care. Manual therapy can complement it but shouldn't replace active treatment.

Alternative treatments besides surgery
Before considering an operation, several non-surgical options are worth exhausting.
- Topical and oral anti-inflammatories (NSAIDs) for short-term flare control
- Neuropathic pain medication (e.g. gabapentinoids) in selected cases, weighed against side effects
- Epidural steroid injections can provide temporary relief, useful as a bridge to rehab
- Cognitive behavioural therapy and pain education for chronic cases
- Acupuncture: modest evidence, low risk
- Heat, ice, and graded walking programmes
- Weight management and smoking cessation if relevant
Surgery (microdiscectomy, decompression) has a role when conservative care has failed for 6 to 12 weeks, when there is significant neurological deficit, or in true emergencies. Even then, outcomes for elective lumbar surgery vary, and a second opinion can clarify whether the recommended procedure matches the imaging and clinical picture.
When should I see a doctor about my pinched nerve symptoms?
See a clinician promptly if any of the following apply:
- Symptoms have not improved after 4 to 6 weeks of self-care
- Pain is severe and disrupting sleep or daily function
- Leg weakness is present or worsening
- Numbness is spreading
- You have a history of cancer, recent infection, unexplained weight loss, or fever
- You're over 50 with new severe back pain
Seek emergency care immediately if:
- You lose control of your bladder or bowels
- You feel numbness in the saddle area (inner thighs, genitals)
- You have sudden, severe weakness in both legs
If surgery has been recommended, it's reasonable, and increasingly common, to seek an independent online second opinion from a spine specialist before proceeding. Many patients I review have non-urgent conditions where rehabilitation has not yet been fully tried.
How much does treatment cost?
Costs vary enormously by country and healthcare system, so I'll keep this general rather than quote specific prices.
- Self-managed care (over-the-counter NSAIDs, walking, online exercise programmes): very low cost
- Physiotherapy: typically the most cost-effective professional intervention
- MRI imaging: moderate cost, often unnecessary in the first 6 weeks
- Epidural injection: higher cost, temporary benefit
- Lumbar discectomy or decompression surgery: substantial cost, plus recovery time off work
- Online second opinion: comparatively low cost, can prevent unnecessary surgery
In most public healthcare systems (NHS, German statutory insurance, and similar), conservative care is covered. The biggest hidden cost of a pinched nerve is usually lost work time, not direct medical fees.
FAQ
Is walking good for a pinched nerve in the lower back?
Yes. Gentle walking is one of the best early activities. It promotes circulation, reduces stiffness, and rarely worsens nerve symptoms. Start with short walks and build up.
Should I get an MRI right away?
Usually no. Guidelines recommend waiting 4 to 6 weeks unless red flags are present. Early MRIs often show incidental findings that lead to unnecessary worry or treatment.
Can sitting make a pinched nerve worse?
Often yes. Sitting increases disc pressure, especially with poor posture. Break up sitting every 30 to 45 minutes, and consider a standing desk during recovery.
Is surgery the only way to get permanent relief?
No. Most people achieve lasting relief without surgery. Surgery is reserved for cases that don't respond to conservative care or have significant neurological involvement.
Can stress make a pinched nerve worse?
Stress doesn't cause the compression, but it amplifies pain perception and muscle tension. Sleep, stress management, and pacing matter.
When is an online second opinion useful?
It's most useful when surgery has been recommended, when you're uncertain about a diagnosis, or when symptoms haven't improved despite treatment. It's not a substitute for in-person evaluation, but it adds an independent perspective.
Conclusion
A pinched nerve in the lower back is uncomfortable, sometimes frightening, but usually not dangerous and rarely requires surgery. The evidence is consistent: stay active within tolerance, prioritise structured rehabilitation, watch for red flags, and give your body time. If a surgeon has recommended an operation and you feel uncertain, that uncertainty is worth taking seriously. Seeking an independent online second opinion is a sensible step before any irreversible decision.
This article is educational and not a substitute for personal medical advice. If your symptoms concern you, please arrange an in-person evaluation with a qualified clinician.