
Last updated: June 21, 2026
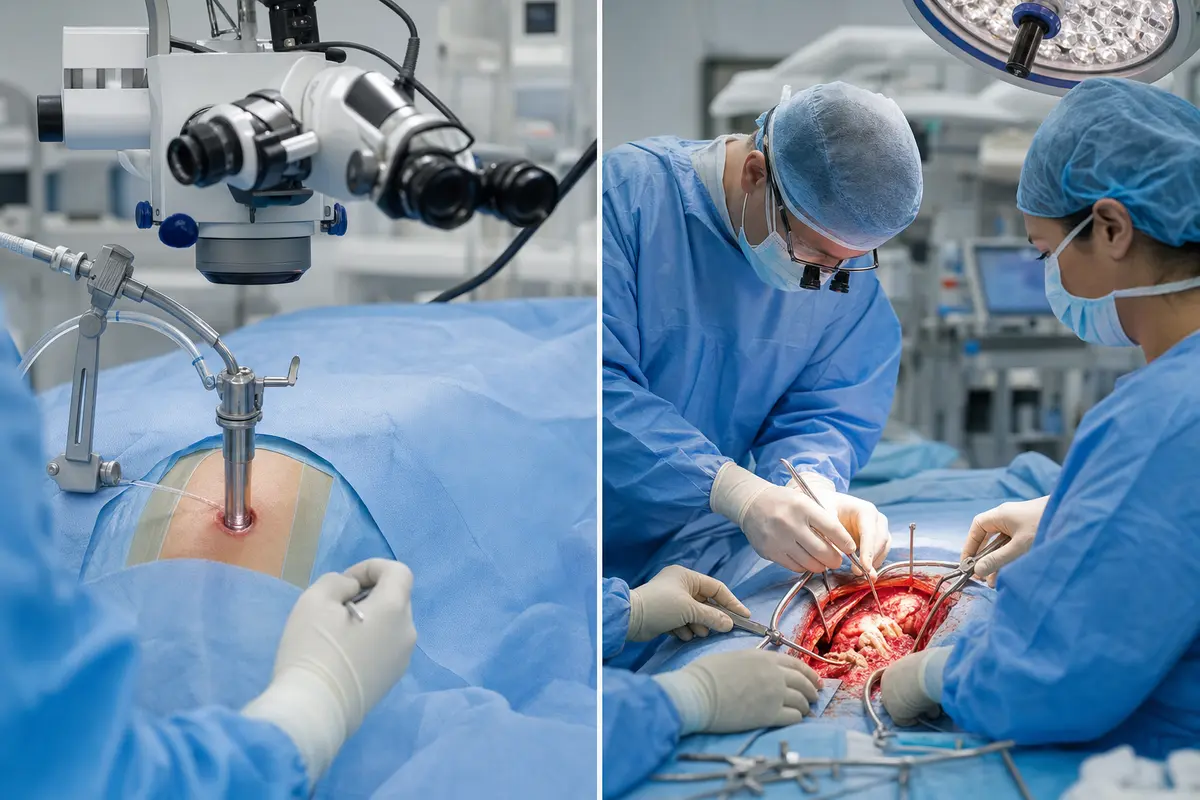
A 4 cm incision or a 15 cm one. A two-night hospital stay or a week. Same diagnosis, sometimes the same surgeon, very different experiences. That's often the gap between minimally invasive and open spine surgery, and it's the question I'm asked most often in my online second opinion consultations: "Can I have the smaller operation instead?"
The honest answer is: sometimes yes, sometimes no, and the difference matters less than most patients think for long-term outcomes. As a board-certified, DWG-certified spine surgeon based in Stolberg, Germany, I want to walk you through what minimally invasive vs open spine surgery actually means, where each one shines, and where the smaller incision is not the right choice. This article is educational and not a substitute for an in-person assessment.
Quick Answer
Minimally invasive spine surgery (MIS) uses small incisions, tubular retractors, and image guidance to reach the spine while sparing muscle and soft tissue. Open spine surgery uses a larger incision and direct visualisation. For many single-level disc or stenosis cases, MIS offers less blood loss, shorter hospital stays, and faster early recovery. For complex deformity, tumours, infections, or multi-level instability, open surgery is often safer and more effective. The best choice depends on your diagnosis, anatomy, and surgeon's experience, not on the size of the scar.
Key Takeaways
- MIS and open surgery often achieve similar long-term outcomes for the right indications.
- MIS typically means less blood loss, less muscle damage, shorter hospital stay, and faster early return to daily activities.
- Open surgery gives wider exposure, which is essential for complex deformity, revisions, tumours, and severe instability.
- Not every patient is a candidate for MIS — anatomy, prior surgery, and pathology all matter.
- Surgeon experience with the specific MIS technique matters more than the marketing label.
- Many spine operations can be safely delayed while you seek a second opinion; emergencies are the exception (cauda equina, progressive weakness, infection, fracture instability).
- An independent second opinion before surgery is reasonable, evidence-supported practice for elective spine procedures.
What is minimally invasive spine surgery?
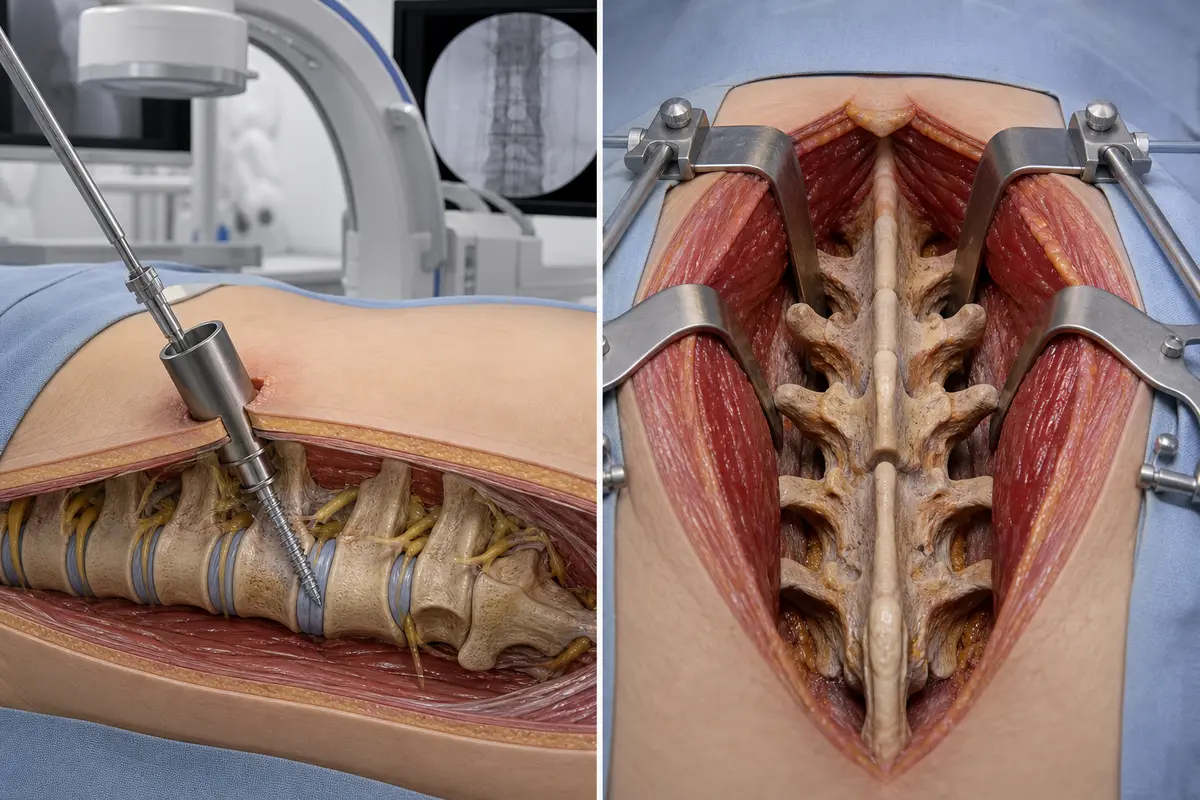
Minimally invasive spine surgery is a group of techniques that access the spine through small incisions, usually 1.5 to 3 cm, using tubular or expandable retractors, an operating microscope or endoscope, and intra-operative imaging such as fluoroscopy or navigation. The goal is to reach the target structure — a disc, nerve root, or vertebra — while disturbing as little muscle and ligament as possible.
Common MIS procedures include:
- Microdiscectomy for a herniated lumbar disc
- Tubular decompression for lumbar spinal stenosis
- MIS TLIF (transforaminal lumbar interbody fusion) for single or two-level instability
- Percutaneous pedicle screw fixation for selected fractures or fusions
- Endoscopic spine surgery through a single small port, often under sedation
MIS is not one operation. It's a philosophy of tissue preservation applied to many different procedures. The technology has matured significantly over the past two decades, and many of the techniques are now considered standard rather than experimental.
What is open spine surgery?
Open spine surgery uses a larger midline or paramedian incision, with the muscles retracted from the bone to give the surgeon a direct, wide view of the spine. It's the traditional approach taught in every spine training programme, and it remains the foundation of spinal surgery worldwide.
Open surgery is often the better — sometimes the only — option when the surgeon needs to:
- Correct a significant deformity (scoliosis, kyphosis)
- Operate on three or more spinal levels
- Remove a tumour or treat a serious infection
- Revise a previous fusion with scar tissue and altered anatomy
- Stabilise complex fractures or treat severe instability
Wider exposure means more control, easier handling of bleeding, and the ability to feel landmarks directly. For complex pathology, that control is worth the larger incision.
Minimally invasive vs open spine surgery: how do they actually compare?
For straightforward, single-level problems, MIS and open surgery produce broadly similar long-term results in terms of pain relief and function. The differences mostly show up in the first weeks to months after surgery.
Here is a practical comparison based on published spine surgery literature and clinical experience:
The size of the scar is not the size of the operation. A small incision over the wrong target helps no one.
The most important point: outcome equivalence depends on choosing the right operation for the right patient. A poorly indicated MIS fusion is not better than a well-indicated open fusion.
When is MIS the better choice?
MIS tends to be the preferred approach when the pathology is focal, the anatomy is favourable, and the surgical goal can be fully achieved through a small corridor. Good candidates often include:
- A single-level lumbar disc herniation with clear nerve compression
- Focal lumbar spinal stenosis at one or two levels
- Single-level degenerative spondylolisthesis without major deformity
- Selected cervical disc herniations (anterior approaches are inherently small-incision)
- Some thoracic disc problems where avoiding a large thoracotomy matters
Choose MIS if: your pathology is localised, your anatomy is straightforward, and your surgeon performs that specific MIS procedure regularly — not occasionally.
When is open surgery the better choice?
Open surgery remains the safer, more effective choice in several common scenarios:
- Adult spinal deformity requiring multi-level correction
- Revision surgery with significant scar tissue
- Spinal tumours needing wide resection
- Spinal infections requiring thorough debridement
- Unstable or complex fractures, particularly with neurological involvement
- Severe multi-level stenosis where wide decompression is needed
- Unfavourable anatomy: very high BMI, unusual bony anatomy, or previous instrumentation in the way
Choose open if: the problem spans multiple levels, requires three-dimensional correction, or involves anatomy that's hard to navigate through a narrow tube.
A common mistake I see in second opinion requests: a patient is told they "must" have MIS because it's modern, when their pathology genuinely needs the exposure of an open approach. Modern does not automatically mean better for your specific case.
How does recovery differ between minimally invasive vs open spine surgery?
Early recovery is usually faster with MIS; long-term recovery is largely driven by the underlying problem, the operation performed, and your rehabilitation, not by incision size.
Typical patterns (these are general ranges, not promises):
Minimally invasive (e.g., microdiscectomy, tubular decompression):
- Walking the same day or next day
- Discharge within 1–3 days
- Light desk work in 1–3 weeks
- Return to physical work or sport in 6–12 weeks
Open (e.g., multi-level decompression or fusion):
- Walking with assistance day 1–2
- Discharge within 3–7 days
- Light desk work in 4–8 weeks
- Return to physical work in 3–6 months
- Bony fusion typically continues maturing for 6–12 months
Pain control, early mobilisation, and structured physiotherapy matter more for your final result than whether the incision was 2 cm or 12 cm. I tell patients honestly: a well-done open operation followed by good rehab usually beats a poorly chosen MIS operation followed by no rehab.

What are the risks and limits of MIS?
MIS is not risk-free, and it has specific limitations worth understanding:
- Steeper learning curve — outcomes correlate strongly with surgeon volume and experience
- Higher intra-operative radiation from fluoroscopy, unless navigation is used
- Limited exposure can make unexpected bleeding or anatomical surprises harder to manage
- Longer operating times in some procedures, especially early in a surgeon's experience
- Equipment-dependent — requires specific retractors, microscopes, endoscopes, and imaging
- Not always feasible in revision cases, severe deformity, or very obese patients
- Conversion to open is sometimes necessary mid-operation; this is a safety decision, not a failure
A patient-centred surgeon will tell you honestly when MIS is unlikely to give you a meaningful advantage, and will not push a technique just because it's the one they market.
Should I get a second opinion before deciding?
For elective spine surgery, yes — a second opinion is reasonable and often valuable. International bodies including NICE and various national spine societies support shared decision-making for elective spine procedures, and published research consistently shows that second opinions change the surgical recommendation in a meaningful minority of cases.
An independent second opinion can help you:
- Confirm the diagnosis matches the imaging and symptoms
- Understand whether non-surgical options have been fully tried
- Compare MIS vs open options for your specific case
- Clarify realistic expectations for recovery and outcome
- Reduce decisional regret
Online second opinions are especially useful when geography or access limits your choices. They are not a replacement for an in-person examination, but they are a useful additional perspective before a major, often irreversible, decision. Emergencies — severe progressive weakness, loss of bladder or bowel control, signs of cauda equina, spinal infection, or unstable fracture — need immediate in-person care, not a second opinion delay.
FAQ
Is minimally invasive spine surgery always better than open surgery?
No. MIS often offers faster early recovery for the right indications, but open surgery is safer and more effective for complex deformity, multi-level disease, tumours, infections, and many revisions. The right operation depends on your diagnosis, not on incision size.
Will I have less pain after MIS?
Usually yes in the first weeks, because less muscle is disturbed. Long-term pain depends on the underlying problem and whether the operation addressed it correctly.
Can every disc herniation be treated with MIS?
Most lumbar disc herniations can be treated with microdiscectomy or endoscopic techniques. Some, particularly large central herniations with significant instability, may need a different approach.
Is endoscopic spine surgery the same as MIS?
Endoscopic spine surgery is one type of MIS. It uses a small camera through a single port, often under sedation. MIS is the broader category, including tubular and microscopic techniques.
How do I know if my surgeon is experienced in MIS?
Ask directly: how many of this specific procedure they perform per year, their conversion-to-open rate, and their complication rate. Experienced surgeons answer these questions openly.
Can I get an online second opinion if I live outside Germany?
Yes. I provide online second opinions internationally as an educational review of your imaging, history, and proposed treatment. It does not replace in-person care but can clarify whether surgery is needed and which approach makes sense.
Conclusion
Minimally invasive vs open spine surgery is not a contest with one winner. They are different tools, and the best surgeons use both, choosing based on what your spine actually needs. MIS can offer real advantages in early recovery for the right cases. Open surgery remains essential — and often superior — for complex problems. Long-term outcomes for well-chosen procedures are broadly similar.
If you've been recommended spine surgery and you're not certain, take these steps:
- Get clear written answers on your diagnosis, the proposed procedure, and the alternatives.
- Ask why MIS or open is being recommended for your specific case.
- Confirm that non-surgical options have been adequately tried, where appropriate.
- Consider an independent second opinion, especially for elective cases.
- Make sure your decision is based on your pathology and your surgeon's experience — not on the marketing of a particular technique.
Your spine deserves the right operation, not just the smallest incision. If you'd like an independent educational review of your case before deciding, an online second opinion is a sensible step.