

Quick Answer: Lumbar radiculopathy is a condition where a spinal nerve root in the lower back becomes compressed or irritated, typically by a herniated disc or bone spur. It causes pain, numbness, or weakness that travels down one leg. The good news: most cases improve within 6 to 12 weeks with conservative treatment, and surgery is only necessary for a minority of patients. If you've been told you need an operation, getting an independent second opinion is a reasonable and often wise step.
Key Takeaways
- Lumbar radiculopathy refers to nerve root compression in the lower back, not a disease in itself but a symptom pattern with a specific cause.
- The most commonly affected levels are L4-L5 and L5-S1, which together account for the vast majority of cases.
- "Sciatica" is a symptom of lumbar radiculopathy, not a separate diagnosis.
- Around 85–90% of patients improve without surgery when managed with physiotherapy, activity modification, and time.
- Red flag symptoms (loss of bladder/bowel control, progressive leg weakness) require urgent medical attention and sometimes emergency surgery.
- MRI is the gold-standard imaging test, but clinical examination remains essential because many people have disc abnormalities on MRI without any symptoms.
- Surgery (most commonly microdiscectomy) is effective when conservative care fails after 6–12 weeks, but it should be a shared decision, not a rushed one.
- An online second opinion from an independent spine specialist can help you understand whether surgery is truly indicated in your case.
What Exactly Is Lumbar Radiculopathy and How Does It Affect My Spine?
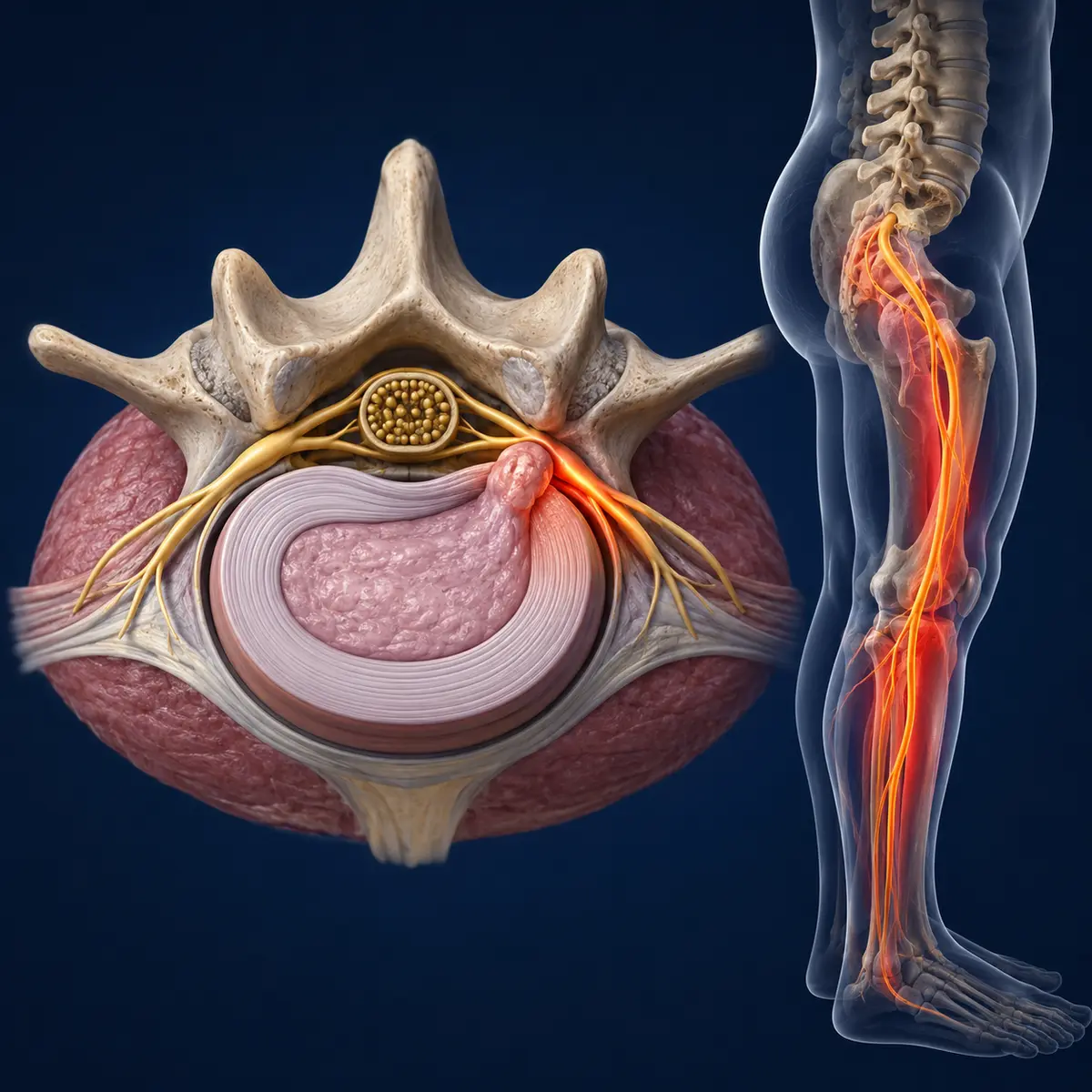
Lumbar radiculopathy is the medical term for a pinched or irritated nerve root in the lumbar (lower back) region of the spine. It is not a disease on its own but rather a clinical syndrome caused by compression, inflammation, or injury to one or more spinal nerve roots as they exit the spinal canal.
Your lumbar spine consists of five vertebrae (L1 through L5), separated by intervertebral discs that act as shock absorbers. Nerve roots branch off the spinal cord and exit through small openings called foramina. When something narrows that space — a herniated disc, a bone spur from arthritis, or spinal stenosis — the nerve root gets squeezed. This triggers pain, altered sensation, or weakness in the area of the body that nerve supplies.
The most commonly affected levels are:
In my practice in Stolberg, Germany, L5-S1 and L4-L5 herniations are by far the most frequent causes I see. Together, these two levels account for roughly 95% of lumbar disc herniations that cause radiculopathy.
How Is Lumbar Radiculopathy Different from Sciatica?
Sciatica is a symptom; lumbar radiculopathy is the underlying clinical diagnosis. Many patients use these terms interchangeably, but they are not the same thing.
"Sciatica" describes pain that travels along the sciatic nerve — from the lower back through the buttock and down the back of the leg. It is the most recognisable symptom of lumbar radiculopathy affecting the L5 or S1 nerve roots. However, lumbar radiculopathy can also affect the L4 or L3 nerve roots, producing pain in the front of the thigh rather than the classic sciatic distribution.
Think of it this way: all sciatica is a form of lumbar radiculopathy, but not all lumbar radiculopathy presents as sciatica. The distinction matters because treatment depends on identifying which nerve root is affected and why.
Why Do I Have Shooting Pain Down My Leg?
The shooting, burning, or electric-shock-like pain that radiates down your leg occurs because the compressed nerve root sends abnormal signals along its entire pathway. This is called "referred" or "radicular" pain.
When a herniated disc presses on a nerve root, it causes both mechanical compression and a local chemical inflammatory response. Substances released from the damaged disc irritate the nerve, amplifying the pain signal. This is why even a small disc herniation can cause severe leg pain — it's not just about pressure, it's about inflammation.
Key characteristics of radicular leg pain include:
- It typically follows a specific pattern (dermatome) depending on which nerve root is affected
- It often feels worse than the back pain itself
- Coughing, sneezing, or straining can intensify it
- Sitting for prolonged periods usually makes it worse
- It may be accompanied by tingling, numbness, or weakness
Who Is Most Likely to Develop Lumbar Radiculopathy?
People between the ages of 30 and 50 are most commonly affected, with men slightly more often than women. However, lumbar radiculopathy can occur at any age.
Risk factors include:
- Sedentary lifestyle — weak core muscles place more load on the discs
- Obesity — excess body weight increases disc pressure
- Smoking — reduces blood flow to the discs, accelerating degeneration
- Occupations involving heavy lifting, twisting, or prolonged sitting
- Genetic predisposition — disc degeneration has a significant hereditary component
- Previous lumbar disc problems
Can Athletes or People with Active Jobs Get Lumbar Radiculopathy?
Absolutely. Athletes in sports involving repetitive spinal loading (weightlifting, gymnastics, football, rowing) are at increased risk. Similarly, manual labourers, nurses, and anyone whose work involves frequent bending, lifting, or vibration exposure can develop this condition. Paradoxically, both too little and too much physical activity can contribute — the key is balanced, appropriate loading of the spine.
What Diagnostic Tests Are Used to Confirm Lumbar Radiculopathy?
The diagnosis of lumbar radiculopathy is primarily clinical, meaning it starts with a thorough history and physical examination. Imaging and electrodiagnostic tests then confirm the suspected cause and level.
Step-by-step diagnostic approach:
- Clinical history — location of pain, onset, aggravating/relieving factors, any bladder or bowel changes
- Physical examination — straight leg raise test (positive in L5/S1 radiculopathy), neurological assessment of reflexes, sensation, and muscle strength
- MRI of the lumbar spine — the gold-standard imaging study; shows disc herniations, nerve root compression, and other soft tissue pathology without radiation
- CT scan — useful when MRI is contraindicated (e.g., certain pacemakers) or for assessing bony pathology
- Nerve conduction studies/EMG — sometimes used when the diagnosis is unclear or to differentiate radiculopathy from peripheral neuropathy
A critical point I emphasise to every patient: MRI findings must be correlated with your symptoms and examination. Studies published in peer-reviewed journals have consistently shown that a significant proportion of people without any back pain have disc bulges or herniations visible on MRI. An abnormal scan alone is never a reason for surgery.
How Long Does It Take to Recover from Lumbar Radiculopathy?
Most patients experience significant improvement within 6 to 12 weeks. The natural history of lumbar radiculopathy — particularly when caused by a disc herniation — is generally favourable.
Typical recovery timeline:
- Weeks 1–2: Acute pain phase; rest as needed but avoid prolonged bed rest (more than 1–2 days of bed rest can actually slow recovery)
- Weeks 2–6: Gradual improvement with physiotherapy, gentle movement, and pain management
- Weeks 6–12: Most patients see substantial or complete resolution of leg symptoms
- 3–6 months: Continued improvement; some residual symptoms may persist but usually manageable
- Beyond 6 months: If significant symptoms persist, surgical options may be discussed more seriously
Recovery speed varies depending on the severity of compression, your overall health, adherence to physiotherapy, and whether you smoke (smoking genuinely slows nerve healing).

What Exercises Can Help Manage Lumbar Radiculopathy Symptoms?
Specific exercises guided by a qualified physiotherapist can significantly reduce symptoms and speed recovery. The McKenzie method (directional preference exercises) and core stabilisation programmes have the strongest evidence base.
Exercises that often help:
- McKenzie extensions — lying face down and gently pressing up to extend the spine; this can help "centralise" leg pain (move it closer to the back, which is a positive sign)
- Nerve gliding/flossing — gentle movements that mobilise the irritated nerve without stretching it aggressively
- Core stabilisation — targeting the deep stabilising muscles (transversus abdominis, multifidus) rather than just the superficial "six-pack" muscles
- Walking — one of the simplest and most effective activities during recovery
- Gentle swimming or aquatic therapy — buoyancy reduces spinal load
Exercises to avoid during the acute phase:
- Heavy deadlifts or squats
- Sit-ups or crunches (increase disc pressure)
- Toe touches or aggressive hamstring stretches
- Any exercise that significantly increases your leg pain
Common mistake: Pushing through sharp, radiating leg pain during exercise. Mild discomfort is acceptable, but if an exercise sends shooting pain down your leg, stop and modify your approach. Pain is information, not something to ignore.
What Alternative Treatments Exist Besides Surgery?
Surgery is only one option, and for most people with lumbar radiculopathy, it is not the first or even the second line of treatment. A structured conservative approach resolves symptoms in the majority of cases.
Evidence-supported conservative treatments:
- Physiotherapy — the cornerstone of non-surgical management
- Oral medications — NSAIDs (ibuprofen, naproxen) for inflammation; short courses of muscle relaxants if needed; neuropathic pain agents (gabapentin, pregabalin) for persistent nerve pain
- Epidural steroid injections — can provide temporary relief (weeks to months) and are most useful as a bridge to allow participation in physiotherapy
- Activity modification — avoiding aggravating postures and movements while staying as active as tolerable
- Manual therapy — spinal mobilisation by a trained physiotherapist or osteopath (avoid aggressive manipulation during the acute phase)
- Acupuncture — some patients report benefit; evidence is mixed but it is generally safe
- Cognitive behavioural approaches — particularly useful for patients with chronic pain or significant fear-avoidance behaviour
What about "alternative" treatments with weaker evidence?
Treatments like spinal decompression tables, laser therapy, and various supplements are widely marketed but lack strong evidence from randomised controlled trials. I don't dismiss them outright, but I encourage patients to be cautious about spending significant money on unproven therapies, especially when effective evidence-based options are available.
What Are the Most Common Mistakes People Make When Treating Lumbar Radiculopathy?
In my experience reviewing cases from around the world through online second opinions, I see several recurring errors:
- Complete bed rest for more than 2 days — this weakens muscles and can prolong recovery. Gentle movement is almost always better.
- Rushing to surgery too quickly — unless red flags are present, conservative treatment deserves a fair trial of at least 6–8 weeks.
- Ignoring red flag symptoms — on the other end, some patients delay seeking help when they have progressive weakness or bladder/bowel changes, which can lead to permanent nerve damage.
- Relying solely on imaging — "My MRI shows a herniation, so I need surgery" is a common but flawed assumption. Many herniations are incidental findings.
- Not engaging with physiotherapy — passive treatments (massage, heat packs, ultrasound) alone are rarely sufficient. Active rehabilitation is essential.
- Fear-avoidance — becoming so afraid of movement that deconditioning sets in, creating a vicious cycle of pain and disability.
How Much Does Treatment for Lumbar Radiculopathy Typically Cost?
Treatment costs vary enormously depending on your country, healthcare system, and whether you pursue conservative or surgical management. I cannot give precise universal figures, but here is a general framework:
In countries with public healthcare systems (UK NHS, German statutory insurance, many others), much of this is covered. In private or out-of-pocket settings, costs can be substantially higher. The key financial point: a second opinion costing a few hundred euros could potentially save you from an unnecessary surgery costing thousands — and more importantly, from the risks that come with any operation.
Can Lumbar Radiculopathy Be Permanently Cured?
Many patients achieve complete and lasting resolution of symptoms, but "permanent cure" depends on the underlying cause. A disc herniation that resolves (the body can actually reabsorb herniated disc material over time) may never recur. However, the degenerative process in the spine continues throughout life, so new problems can develop at the same or different levels.
Realistic expectations:
- Most acute episodes of lumbar radiculopathy caused by disc herniation resolve fully
- Some patients have recurring episodes, particularly if risk factors (obesity, smoking, sedentary lifestyle) are not addressed
- Surgery can effectively relieve nerve compression, but it does not reverse underlying disc degeneration
- Long-term spinal health depends on ongoing core strengthening, weight management, and activity
When Should I See a Doctor About My Lumbar Radiculopathy Symptoms?
You should seek medical evaluation if leg pain persists beyond 2–4 weeks despite basic self-care, or immediately if you develop any red flag symptoms.
Seek urgent or emergency care if you experience:
- Loss of bladder or bowel control (inability to urinate or incontinence)
- Saddle anaesthesia (numbness in the groin/inner thigh area)
- Rapidly progressive weakness in one or both legs
- Severe, unrelenting pain that does not respond to any position change or medication
These symptoms may indicate cauda equina syndrome, a surgical emergency. Delay in treatment can result in permanent neurological damage.
See a doctor soon (within days) if you have:
- Leg pain that is worsening rather than improving
- Significant numbness or tingling that interferes with daily function
- Difficulty walking or a foot that "slaps" when you step (foot drop)
- Pain that disrupts sleep consistently
For everything else — mild to moderate symptoms that are gradually improving — it is reasonable to start with conservative measures and seek evaluation if there is no improvement after a few weeks.
Frequently Asked Questions
Is lumbar radiculopathy the same as a slipped disc?
Not exactly. A "slipped disc" (more accurately, a herniated disc) is one common cause of lumbar radiculopathy, but radiculopathy can also be caused by spinal stenosis, bone spurs, spondylolisthesis, or other conditions that compress a nerve root.
Can lumbar radiculopathy cause permanent nerve damage?
In most cases, no. However, prolonged severe compression — particularly if associated with cauda equina syndrome or progressive motor weakness — can lead to lasting nerve injury. This is why red flag symptoms should never be ignored.
Do I need surgery for lumbar radiculopathy?
Most people do not. Conservative treatment is effective for the majority. Surgery is typically considered when significant symptoms persist beyond 6–12 weeks of appropriate conservative care, or when there is progressive neurological deficit. If surgery has been recommended, an independent second opinion can help you make an informed decision.
Is it safe to exercise with lumbar radiculopathy?
Yes, with appropriate guidance. Gentle, controlled exercise is one of the best things you can do. Avoid high-impact activities and exercises that worsen your leg pain. A physiotherapist experienced in spinal conditions can design a safe programme for you.
Can lumbar radiculopathy go away on its own?
Yes. Many cases, especially those caused by disc herniations, improve significantly or resolve completely within weeks to months without any intervention beyond basic pain management and activity modification.
Should I get a second opinion before spine surgery?
I strongly encourage it. Spine surgery is a significant decision, and studies consistently show that surgical recommendations vary between surgeons. An independent second opinion — whether in person or online — gives you additional perspective and confidence in your treatment plan. This is especially valuable if you live in an area with limited access to subspecialised spine surgeons.
Conclusion
Lumbar radiculopathy is common, often frightening, but usually manageable without surgery. Understanding your diagnosis — which nerve is affected, what's causing the compression, and what the realistic timeline for recovery looks like — puts you in a much stronger position to make good decisions about your care.
Actionable next steps:
- If you have new symptoms, see a qualified clinician for a proper examination and, if indicated, an MRI.
- Start structured physiotherapy early — it is the single most effective conservative intervention.
- Give conservative treatment a fair trial (at least 6–8 weeks) unless red flag symptoms are present.
- If surgery has been recommended, consider seeking an independent second opinion. As a spine surgeon who provides online second opinions to patients worldwide, I can tell you that a significant proportion of the cases I review have viable non-surgical options that were not fully explored.
- Address modifiable risk factors: stop smoking, maintain a healthy weight, and stay physically active.
Your spine is more resilient than you might think. Most disc herniations improve with time and the right support. Surgery is an excellent tool when truly needed, but it should be the last option considered, not the first.
This article is for educational purposes and does not constitute personal medical advice. Individual cases vary, and an in-person evaluation by a qualified specialist is recommended for diagnosis and treatment planning.