
Last updated: June 16, 2026
Quick Answer
Laminectomy removes a small piece of bone (the lamina) to take pressure off compressed nerves, while spinal fusion permanently joins two or more vertebrae together using screws, rods, and bone graft. For most patients with nerve compression from spinal stenosis or a disc problem, decompression alone is enough — fusion is only needed when the spine is genuinely unstable, deformed, or when significant bone must be removed to free the nerves. Before agreeing to fusion, it's worth getting an independent second opinion, because adding fusion when it isn't required exposes you to bigger surgery and long-term stiffness without extra benefit.
Key Takeaways
- Laminectomy is a decompression procedure: it relieves pressure on nerves without changing the structure of the spine.
- Spinal fusion permanently locks vertebrae together and is reserved for instability, deformity, or recurrent problems at the same level.
- For lumbar spinal stenosis without instability, high-quality evidence (including the SPORT trial and Försth et al., NEJM 2016) suggests adding fusion to decompression often does not improve outcomes.
- Recovery from laminectomy alone is typically faster, less painful, and preserves more motion.
- Fusion carries a higher risk of complications, longer rehabilitation, and adjacent segment disease years later.
- A second opinion is reasonable any time fusion is recommended, especially for "just-in-case" stability concerns.
- Surgery is rarely an emergency: most spinal conditions allow time for proper evaluation and a non-surgical trial first.
What exactly is a laminectomy and how is it different from spinal fusion?
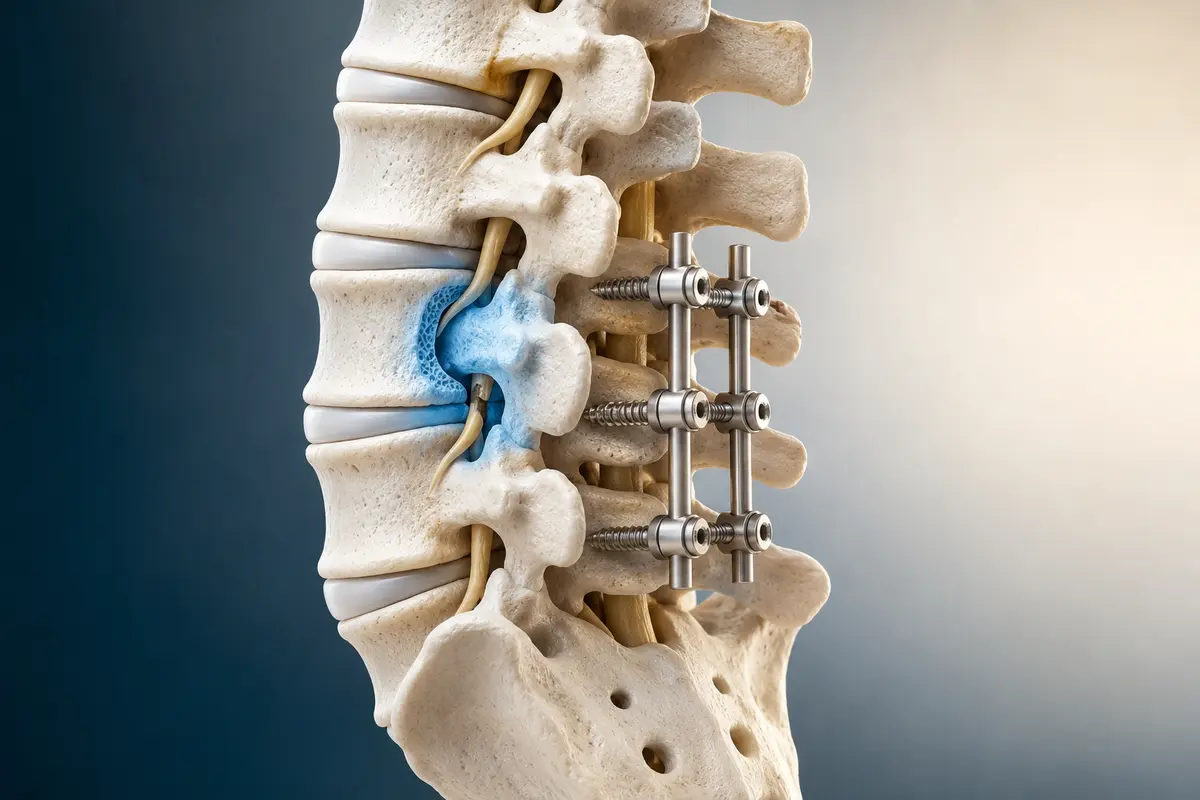
A laminectomy removes part of the lamina — the bony arch at the back of a vertebra — to create more space for compressed nerves. A spinal fusion is a structural operation that joins two or more vertebrae using bone graft and usually metal hardware (pedicle screws and rods or interbody cages), so they grow together into one solid unit.
The distinction matters because the two procedures solve different problems:
- Laminectomy treats nerve compression. Think of it as opening a tight tunnel so the nerve can breathe.
- Fusion treats instability or deformity. It stops painful, abnormal movement between vertebrae.
A common point of confusion: a laminectomy can be done as part of a fusion (to access the nerves), but a laminectomy on its own does not involve any hardware, screws, or bone graft. Many patients I review online have been told they need "a laminectomy and fusion" when, on closer inspection of their imaging and symptoms, the fusion part may not be necessary.
Which surgery is better for lower back pain?
Neither surgery is a reliable treatment for pure lower back pain. Both are designed primarily to treat leg pain, numbness, or weakness caused by nerve compression, or to stabilise a clearly unstable spine.
If your dominant problem is axial back pain without leg symptoms and without clear instability on imaging, evidence for either operation is weak. NICE guidance (NG59) on low back pain and sciatica emphasises that surgery is appropriate when:
- There is clear radicular pain (sciatica) or neurogenic claudication that matches the imaging, and
- Non-surgical treatment over a reasonable period has not helped, or there are progressive neurological signs.
Decision rule: if a surgeon offers fusion mainly to "treat your back pain" and your MRI does not show instability, spondylolisthesis with movement, deformity, or fracture, ask for a second opinion before committing.
How much does a laminectomy cost compared to fusion surgery?
Costs vary widely by country and healthcare system, but the pattern is consistent everywhere: fusion is substantially more expensive than laminectomy alone — often two to four times more — because of implants, longer operating time, longer hospital stay, and longer rehabilitation.
I won't quote specific prices because they differ enormously between Germany, the UK, the US, the Gulf, and Asia, and they depend on public vs private care. The point is that the financial and biological cost of fusion is real, and that's another reason to be sure it's actually needed.
What are the recovery times for each procedure?
Most patients walk the same day after a laminectomy and return to light work within 4 to 6 weeks. After a one- or two-level fusion, walking starts the next day, but full bony fusion takes 3 to 12 months, and return to heavier activity is typically delayed to 3 to 6 months or longer.
A realistic recovery timeline:
- Laminectomy: hospital 1–3 nights, walking immediately, driving in 2–4 weeks, desk work in 2–4 weeks, physical work in 6–12 weeks.
- Fusion (1–2 levels): hospital 2–5 nights, restrictions on bending/lifting/twisting for several weeks, gradual loading over 3–6 months, bone healing completing by 6–12 months.
Recovery is also more variable after fusion. Smoking, diabetes, osteoporosis, and obesity all measurably slow bone healing and raise complication rates.

Risks and complications of laminectomy vs fusion
Both are generally safe operations in experienced hands, but the risk profile is meaningfully higher for fusion. Laminectomy carries small risks of infection, dural tear (CSF leak), bleeding, and recurrent symptoms. Fusion adds risks tied to hardware and biology: pseudarthrosis (failure to fuse), screw malposition, blood loss, and adjacent segment disease, where the levels above or below the fusion wear out faster.
"Every level you fuse is a level you can never move again. That trade-off is sometimes absolutely worth it — and sometimes it isn't. The job of a good spine consultation is to tell you honestly which one you are."
Published series and registry data (e.g. Swedish Spine Register, Spine Tango) consistently show higher complication and reoperation rates for instrumented fusion compared with decompression alone, even when patient profiles are matched.
Who is a good candidate for laminectomy alone?
The classic candidate is a patient with lumbar spinal stenosis causing neurogenic claudication — leg pain, heaviness, or numbness when walking, relieved by sitting or leaning forward — with imaging that confirms central or lateral recess narrowing without significant instability.
Good signs that decompression alone is appropriate:
- Leg-dominant symptoms (more leg than back pain).
- MRI shows stenosis, disc herniation, or facet hypertrophy compressing nerves.
- No or only minimal spondylolisthesis (typically <4–5 mm and not moving on flexion-extension X-rays).
- No scoliosis or deformity at the affected level.
- Reasonable bone quality and overall health.
In these patients, a focused decompression — open, microsurgical, or minimally invasive — often gives excellent leg-symptom relief while preserving spinal motion.
When do doctors recommend spinal fusion instead of laminectomy?
Fusion is genuinely indicated when the spine is mechanically unstable, deformed, or when a thorough decompression would itself destabilise the spine. The clearest indications include:
- Spondylolisthesis with documented motion (especially symptomatic grade I–II isthmic or degenerative slips that slide on dynamic X-rays).
- Significant scoliosis or kyphosis contributing to symptoms.
- Recurrent disc herniation at the same level after multiple decompressions.
- Fractures, tumours, or infections compromising structural integrity.
- Wide bilateral facetectomy required to decompress, leaving the segment unstable.
When none of those apply, the case for adding fusion to decompression weakens considerably. The landmark Swedish trial by Försth et al. (NEJM, 2016) found that in patients with lumbar stenosis (with or without degenerative spondylolisthesis), adding fusion to decompression did not improve clinical outcomes at 2 or 5 years but did increase cost, blood loss, and operating time.
What conditions require spinal fusion versus laminectomy?
A simple way to think about it:
Conditions that rarely need fusion as a first step: simple disc herniation, single-level stenosis without slip, and isolated facet arthritis.
Can I avoid surgery and treat my spinal condition another way?
Yes — for most degenerative spinal conditions, non-surgical care is the right first step, and many people improve without ever needing an operation. Surgery is mainly indicated for persistent radicular pain, neurogenic claudication that limits walking, or progressive neurological deficit.
Evidence-supported non-surgical options include:
- Structured physiotherapy focused on core stability, hip mobility, and graded activity.
- Activity modification rather than bed rest.
- Pain control (NSAIDs where safe, neuropathic agents for nerve pain, short courses of stronger analgesics if needed).
- Targeted spinal injections (e.g. epidural steroid injections) for selected radicular pain.
- Treating contributing factors: weight, smoking, sleep, mood, and deconditioning.
Cochrane reviews on exercise therapy and on surgery vs non-surgical treatment for sciatica and stenosis consistently show that many patients improve with conservative care, and that the gap between surgical and non-surgical outcomes often narrows over 1–2 years for those without severe neurological signs.
Long-term success rates for laminectomy and fusion
Both procedures have good long-term success when the indication is right. For lumbar decompression in well-selected stenosis patients, 60–80% report meaningful, sustained improvement in leg symptoms at 4–10 years (SPORT trial follow-up, Weinstein et al.). For fusion in clear instability (e.g. isthmic spondylolisthesis), satisfaction rates are similarly high.
The picture changes when fusion is done for less clear indications — chronic low back pain without instability, or "preventive" stabilisation around a decompression. In those scenarios, long-term satisfaction drops and reoperation rates climb, particularly from adjacent segment problems appearing 5–10 years later.

How painful is recovery from each type of surgery?
Laminectomy pain is usually moderate for the first 1–2 weeks, with most patients off strong analgesics within 2–3 weeks. Fusion pain is more intense and lasts longer — typically 4–8 weeks of significant discomfort, with muscle pain, hardware-related ache, and graft site soreness on top of the incision itself.
What patients often tell me:
- After laminectomy: "The leg pain was gone when I woke up. The back was sore for a couple of weeks."
- After fusion: "The leg pain was better, but the back stiffness and aching took months to settle."
Multimodal pain protocols, early mobilisation, and good physiotherapy meaningfully improve both experiences.
Common mistakes patients make after laminectomy surgery
The biggest mistakes I see are not in surgery — they're in the weeks afterwards:
- Doing too much, too soon. Feeling great at 2 weeks isn't permission to lift heavy boxes.
- Doing too little, too long. Avoiding all activity leads to deconditioning and chronic pain.
- Skipping physiotherapy because "the leg pain is gone."
- Ignoring red flags: new weakness, bladder/bowel changes, fever, or spreading redness need urgent review.
- Smoking during recovery, which slows healing for both procedures and dramatically reduces fusion success rates.
Potential side effects of spinal fusion that patients should know
Beyond the standard surgical risks, fusion has specific long-term considerations worth understanding before consenting:
- Adjacent segment disease: the level above or below the fusion takes on extra stress and can degenerate faster, sometimes requiring further surgery years later.
- Loss of motion at the fused segment (often less noticeable in the lumbar spine than patients fear, but real).
- Pseudarthrosis: failure of the bone to fuse, which can cause ongoing pain and may require revision.
- Hardware-related symptoms: prominent screws or rods occasionally cause irritation.
- Higher revision rates compared with decompression alone over 5–10 years.
None of these should scare a patient who clearly needs fusion. They should, however, make everyone pause when fusion is being added "just in case."
Why a second opinion matters before agreeing to fusion
If a surgeon has recommended fusion, an independent second opinion is one of the highest-value things you can do — particularly when the recommendation is for back pain alone, mild spondylolisthesis without dynamic instability, or "stabilisation" alongside decompression.
A good second opinion will:
- Re-examine your MRI and, ideally, dynamic (flexion-extension) X-rays.
- Match imaging findings to your actual symptoms.
- Consider whether decompression alone, a smaller operation, or continued non-surgical care is reasonable.
- Be transparent about uncertainty, not promise outcomes.
As an online second-opinion service for international patients, I see cases every week where the answer is "yes, fusion is the right plan" — and others where decompression alone or no surgery at all is more appropriate. Either way, you deserve to know.
FAQ
Is a laminectomy a major surgery?
Yes, it's a real operation under general anaesthesia, but it's considered moderate in scope — typically 1–2 hours, 1–3 nights in hospital, and recovery measured in weeks rather than months.
Can a laminectomy fail and require fusion later?
Sometimes. A small percentage of patients develop instability or recurrent symptoms and may need fusion later, but this is uncommon when the initial indication and surgical technique were appropriate.
Is minimally invasive surgery better than open surgery?
For selected patients, minimally invasive decompression offers less muscle damage and faster recovery with similar long-term results. The choice depends on anatomy and surgeon experience more than marketing.
How long do I have to decide on spine surgery?
For most degenerative conditions, weeks to months. True emergencies (cauda equina syndrome, progressive weakness, fracture with neurological deficit) are rare and obvious. For everything else, there's time for a second opinion.
Will fusion make me stiff?
A one- or two-level lumbar fusion is usually well-tolerated and most patients don't notice major stiffness. Longer constructs, especially crossing into the thoracic spine, are more limiting.
Can I get a spine second opinion online?
Yes. With your MRI images and clinical history, an experienced spine surgeon can review your case remotely and give an educational second opinion before you commit to surgery. This is not a substitute for in-person care but a valuable additional perspective.
Conclusion
The honest answer to "laminectomy vs fusion" is that they're different tools for different problems. Decompression alone solves nerve compression. Fusion solves instability. Mixing them up — or adding fusion when only decompression is needed — is one of the most common avoidable problems in spine surgery today.
If you've been told you need a fusion, here's what I'd suggest as practical next steps:
- Get a clear written explanation of why fusion is being recommended over decompression alone.
- Ask whether dynamic (flexion-extension) X-rays have been done to check for true instability.
- Confirm your symptoms match the imaging findings.
- Consider an independent online or in-person second opinion, especially if fusion is being added "just in case."
- Treat surgery as one option in a broader plan that includes physiotherapy and time, not as the default.
This article is educational and not personal medical advice. Every spine is different, and the right decision depends on your imaging, your symptoms, your goals, and your overall health. A careful, unhurried evaluation — ideally with more than one expert opinion — is almost always the right path before agreeing to a permanent operation.