

Last updated: June 6, 2026
Roughly four out of five adults will deal with significant back pain at some point in their lives, and a meaningful share of them will be offered an injection before anyone seriously discusses surgery. That timing matters. As a spine surgeon who reviews second opinions from patients all over the world, I see the epidural steroid injection for back pain treated as either a miracle or a waste of time — and the truth sits firmly in between.
Quick Answer
An epidural steroid injection for back pain is a fluoroscopy-guided injection of corticosteroid (often combined with a local anaesthetic) into the epidural space around irritated spinal nerves. Evidence shows it provides short-term relief — typically a few weeks to a few months — for radicular pain caused by disc herniation or spinal stenosis. It is best understood as a bridge to physiotherapy and active rehabilitation, and as a tool that may help some patients delay or avoid surgery, not as a long-term cure.
Key Takeaways
- Epidural steroid injections (ESIs) are most effective for leg pain (sciatica/radiculopathy) caused by nerve root inflammation, not for pure axial (mechanical) low back pain.
- Relief is usually short-term (2 weeks to 3 months); some patients get longer benefit, others get none.
- ESIs can be a valuable bridge to physiotherapy, weight loss, and graded activity — which are what change long-term outcomes.
- Serious complications are rare when performed under image guidance by experienced clinicians, but real risks exist.
- An injection that fails is useful diagnostic information — it doesn't automatically mean you need surgery.
- Before any spine surgery, an independent second opinion is reasonable and often clarifying.
What exactly is an epidural steroid injection?
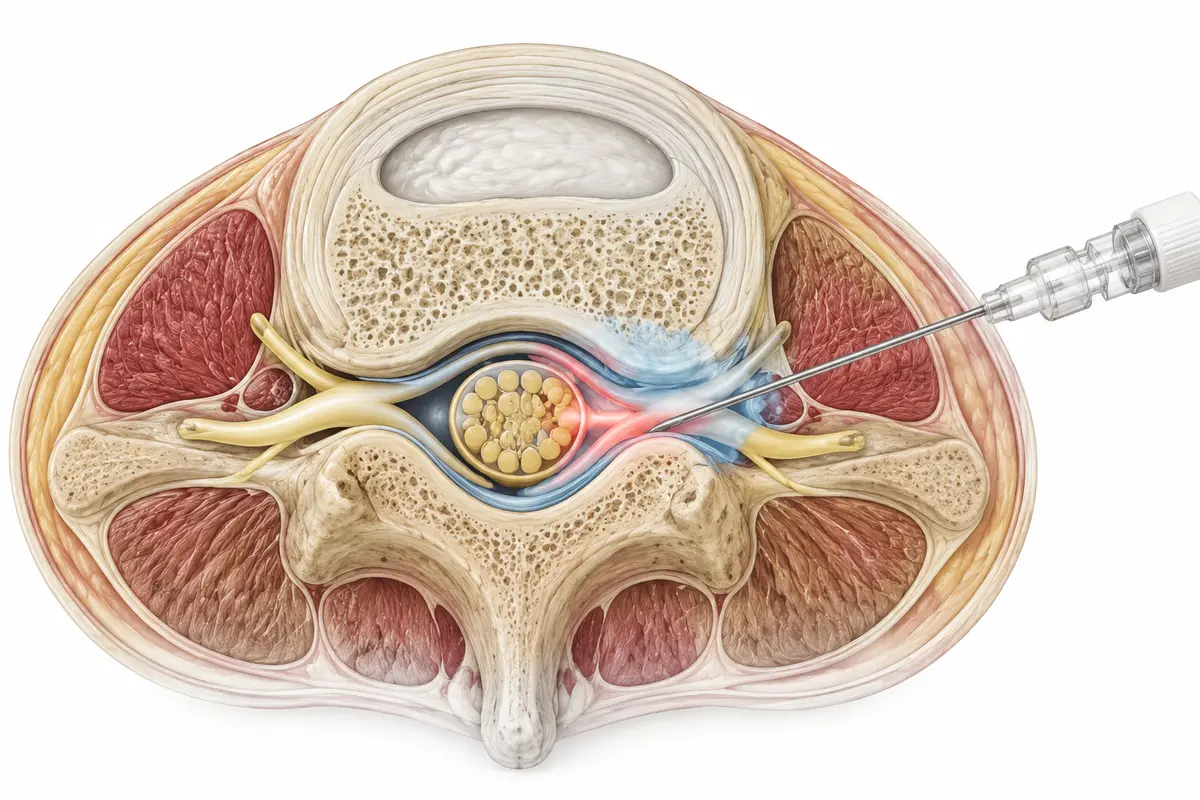
An epidural steroid injection is a minimally invasive procedure in which a clinician places a thin needle into the epidural space — the area just outside the dural sac that surrounds the spinal cord and nerve roots — and delivers a corticosteroid, sometimes mixed with a local anaesthetic. The goal is to reduce inflammation around a compressed or irritated nerve.
There are three common approaches:
- Interlaminar: between two vertebrae from the back.
- Transforaminal: through the nerve root exit foramen, targeting a specific nerve.
- Caudal: through the sacral hiatus at the base of the spine.
Image guidance (fluoroscopy or, less commonly, CT) is the standard of care. Without it, needle placement accuracy drops significantly. Most guidelines, including those from professional pain and spine societies, treat fluoroscopic guidance as expected practice.
What conditions can be treated with this injection?
ESIs target nerve-related (radicular) pain, not generalised back stiffness. They tend to help most when there is a clear inflammatory or compressive cause of nerve pain.
Conditions where ESIs are commonly considered:
- Lumbar disc herniation with radiculopathy (sciatica)
- Cervical disc herniation with arm pain
- Lumbar spinal stenosis with leg symptoms (more modest benefit)
- Foraminal narrowing pressing on a specific nerve root
- Post-surgical radicular pain, in selected cases
Conditions where evidence is weak or unfavourable:
- Pure axial low back pain without leg symptoms
- Degenerative disc disease without nerve compression
- Facet-joint mediated pain (a facet injection or medial branch block is more appropriate)
- Sacroiliac joint pain
Decision rule: if your pain is mainly in your back and not radiating below the knee, an ESI is unlikely to be the right tool.
How long do the pain relief effects typically last?
Most patients who respond experience meaningful relief for two weeks to three months. A smaller subset enjoy longer benefit; some feel little change at all. Cochrane reviews and large systematic reviews consistently describe short-term, modest improvements in pain and function for radicular pain, with diminishing differences from placebo by 6–12 months.
What this means practically:
- ESIs buy time for nature, physiotherapy, and tissue healing to work.
- They are not curative for the underlying disc or stenosis.
- Around 60–70% of lumbar disc herniations improve substantially within 6–12 weeks regardless of treatment; an ESI can make that window tolerable.
What should I expect during and after the procedure?
The procedure itself usually takes 15 to 30 minutes, including positioning and imaging. You lie face down on a fluoroscopy table. The skin is cleaned and numbed. The clinician advances the needle under live X-ray, confirms position with a small amount of contrast dye, and slowly injects the medication.
Typical experience:
- Before: light meal usually fine; stop blood thinners only on your doctor's specific instruction.
- During: mild pressure or a brief twinge of familiar pain when the medication reaches the nerve.
- First 24–48 hours: sometimes a temporary increase in pain as the anaesthetic wears off and before the steroid acts.
- Days 3–7: steroid effect generally begins.
- Follow-up: reassessment at 2–4 weeks to decide on physiotherapy intensity and whether a repeat injection is reasonable.
You can usually walk out the same day and resume light activity within 24 hours.
How is the injection different from other back pain treatments?
An ESI is one tool in a larger toolbox. Here's how it compares:
The point isn't to rank these — it's to match the right tool to the right pain generator.
Am I a good candidate for this procedure?
You're more likely to benefit if you have:
- Leg or arm pain greater than back/neck pain
- A clear MRI finding that explains your symptoms (a disc herniation or foraminal stenosis matching the affected nerve)
- Symptoms lasting more than 4–6 weeks despite conservative care
- No red flags (no bowel/bladder dysfunction, no progressive weakness, no signs of infection or tumour)
You're a poor candidate if your imaging doesn't match your symptoms, your pain is purely axial, or you have an active infection, bleeding disorder, or uncontrolled diabetes.
Who should not get an epidural steroid injection?
ESIs are generally avoided or postponed in patients with:
- Local or systemic infection
- Bleeding disorders or therapeutic anticoagulation that can't be safely paused
- Allergy to contrast dye or the medications used
- Pregnancy (due to fluoroscopy radiation)
- Poorly controlled diabetes (steroids raise blood glucose)
- Cauda equina syndrome or progressive neurological deficit — these need urgent surgical evaluation, not an injection
If you have new weakness in a leg, numbness in the groin, or loss of bladder or bowel control, this is a surgical emergency. Do not wait for an injection appointment — go to A&E.
What are the risks and potential side effects?
Serious complications are uncommon, but honest informed consent matters. Reported risks include:
- Common and minor: temporary increased pain, injection-site soreness, flushing, insomnia, transient blood sugar elevation, brief menstrual irregularities.
- Uncommon: headache from inadvertent dural puncture, transient nerve irritation, vasovagal reaction.
- Rare but serious: epidural haematoma, infection (epidural abscess), nerve injury, and — particularly with transforaminal cervical injections — vascular events.
Repeated steroid exposure can also cause systemic effects: bone density loss, adrenal suppression, and cumulative metabolic impact. Most guidelines suggest no more than 3–4 injections per year, and only if each one provides clear benefit.
How soon can I return to normal activities, and what mistakes do patients make?
Most patients return to desk-based work within 1–2 days and light exercise within a week. The biggest mistake I see is treating the injection as the finish line.
Common post-procedure mistakes:
- Skipping physiotherapy once pain improves — this is exactly when active rehab works best.
- Returning to heavy lifting too early, mistaking pain relief for tissue healing.
- Stacking injections without reassessing whether they're actually helping.
- Ignoring sleep, weight, and smoking — all three significantly influence spine outcomes.
- Assuming a failed injection means surgery is needed. It doesn't, on its own.
Treat the weeks after an ESI as your window of opportunity to rebuild strength, mobility, and confidence.

What are the success rates for different types of back pain?
Reported response rates vary widely across studies, but reasonable estimates from systematic reviews look roughly like this:
- Lumbar disc herniation with radiculopathy: ~50–75% report meaningful short-term relief.
- Lumbar spinal stenosis: ~30–50% short-term relief; benefit over placebo is modest.
- Cervical radiculopathy: ~40–60% meaningful relief in selected patients.
- Axial low back pain alone: generally poor response; not recommended as first-line.
The honest summary: ESIs help a real subset of patients meaningfully in the short term, help a smaller subset for longer, and don't help everyone. They have not been shown to change the long-term natural history of disc disease or stenosis in most trials.
Are there alternatives if this injection doesn't work?
Yes — and a failed ESI is information, not a verdict. Reasonable next steps include:
- Structured physiotherapy with a spine-focused therapist
- Targeted exercise programmes (McKenzie, motor control, graded activity)
- A different injection type (e.g., transforaminal if interlaminar failed, or facet/medial branch block if the pain pattern fits)
- Neuropathic medications (gabapentinoids, certain antidepressants) under medical supervision
- Lifestyle factors: weight, sleep, smoking cessation, stress management
- Surgical consultation if there's a structural problem matching the symptoms and conservative care has truly been exhausted
Before agreeing to surgery, I'd encourage anyone to seek an independent second opinion — ideally one that reviews your MRI alongside your symptoms, not just the images. Many patients I review online turn out to have non-surgical paths still available to them.
How much does an epidural steroid injection cost?
Cost varies widely by country, healthcare system, and whether imaging guidance is included. In many European public systems, ESIs are covered when medically indicated. Privately, prices commonly range from a few hundred to a few thousand euros or pounds per injection, depending on facility fees, imaging, and clinician expertise. I'd suggest asking your provider for a written breakdown — including imaging, medication, and follow-up — before booking.
A balanced view from my practice
When patients send me their MRI for an online second opinion, they often ask: "Should I have the injection or go straight to surgery?" My answer is rarely binary. For radicular pain with a matching disc herniation and no red flags, a well-placed ESI plus committed physiotherapy is a reasonable first step. It can take the edge off long enough for the body to do what it often does — heal. If after one or two injections nothing has changed, and the structural cause is clear, surgery becomes a more honest conversation.
This is general education, not personal medical advice. Decisions about your spine deserve an in-person clinical examination and, when surgery is on the table, ideally a second independent opinion.
FAQ
Is an epidural steroid injection the same as an epidural for childbirth?
No. Both target the epidural space, but the medications, goals, and dosing are different. The labour epidural delivers continuous anaesthesia; the steroid injection delivers anti-inflammatory medication.
How many injections can I safely have?
Most guidelines suggest a maximum of 3–4 per year, only if each provides clear benefit. More than that increases systemic steroid risks without proportionate gain.
Will the injection fix my disc herniation?
No. It reduces inflammation around the nerve. Many disc herniations shrink on their own over months; the injection helps you tolerate that healing window.
Can I drive home afterwards?
Most centres recommend arranging a lift, especially if sedation was used or if local anaesthetic causes temporary leg weakness.
Does a failed injection mean I need surgery?
Not by itself. A failed ESI is one data point. The decision depends on your symptoms, imaging, neurological exam, and how conservative care has been structured.
Is it safe during pregnancy?
Generally avoided because of fluoroscopy radiation. Discuss alternatives with your obstetrician and spine clinician.
Conclusion
The epidural steroid injection for back pain is neither a cure nor a placebo — it's a focused tool for nerve-related pain that, used well, can buy meaningful time for healing and rehabilitation. Treat it as a bridge, not a destination. Pair it with active physiotherapy, address sleep and weight, and reassess honestly at 4–6 weeks.
If surgery has been recommended to you, take a breath. Confirm the diagnosis matches the imaging. Ask whether a structured non-surgical trial has truly been completed. And if anything feels rushed or unclear, consider an independent online second opinion before committing to an operation. Spines deserve careful thinking, not pressured decisions.