

Last updated: June 22, 2026
Quick Answer
Endoscopic spine surgery is a minimally invasive technique that uses a pencil-thin tube with a camera and light to treat specific spinal problems, most often a herniated lumbar disc pressing on a nerve. It is performed through an incision of roughly 7–10 mm, often under sedation rather than general anaesthesia, and most patients walk the same day. It is not suitable for every spine condition, however, and choosing it should depend on your diagnosis, not the marketing around the technology.
Key Takeaways
- Endoscopic spine surgery uses a small tubular endoscope (around 7 mm) to remove disc fragments or decompress nerves through a tiny skin incision.
- The best evidence supports it for contained lumbar disc herniations and selected foraminal stenosis; results compare favourably with traditional microdiscectomy in well-selected patients.
- It is not a fix for every spine problem. Significant instability, severe multilevel stenosis, deformity, or large central herniations often need a different approach.
- Most patients go home the same day, return to desk work within 1–2 weeks, and resume heavier activity by 6–12 weeks.
- Surgeon experience matters enormously — the learning curve is steep, and outcomes are operator-dependent.
- Before agreeing to any spine operation, an independent second opinion (in person or online) is reasonable and often clarifying.
- This article is educational. It does not replace a personal evaluation by a qualified spine surgeon.
What Is Endoscopic Spine Surgery?
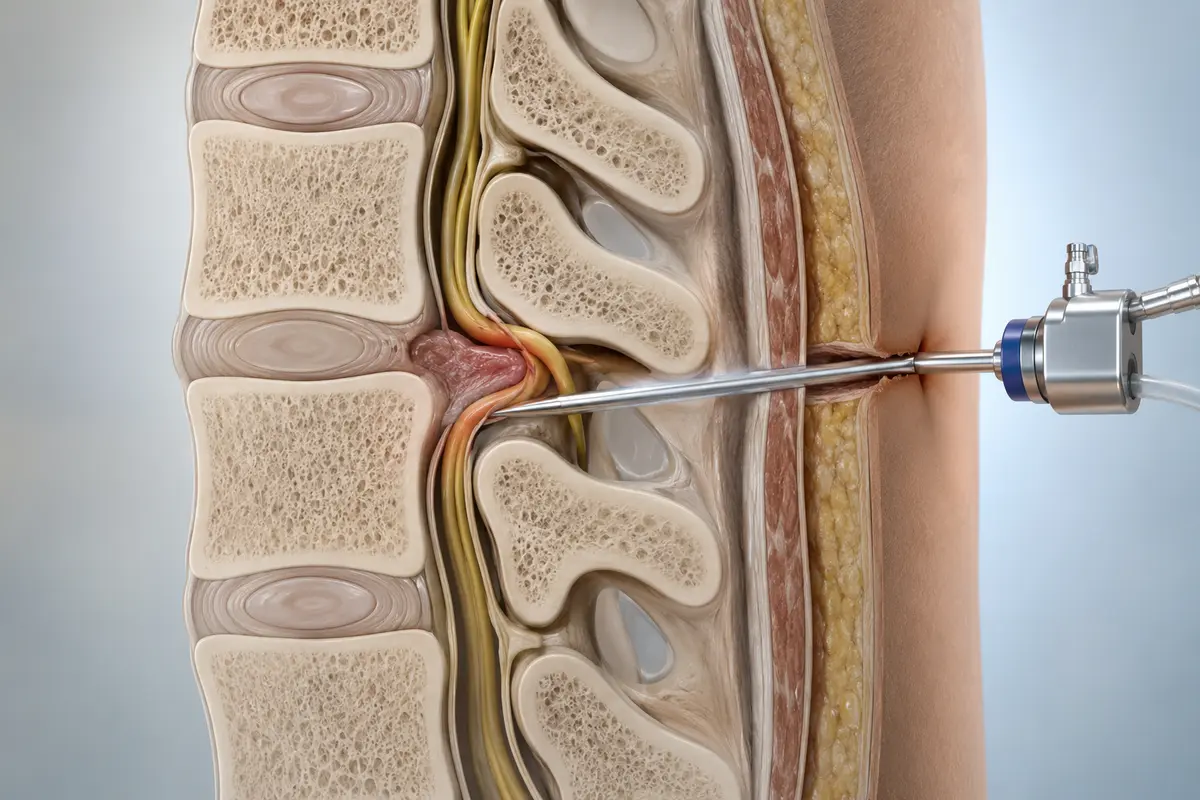
Endoscopic spine surgery is a category of minimally invasive procedures in which a surgeon works through a narrow tube (the endoscope) fitted with a high-definition camera, a light source, and a working channel for tiny instruments. Saline irrigation keeps the field clear, and the entire operation is performed while watching a magnified video monitor.
The two most common approaches are:
- Transforaminal — the endoscope enters from the side, through the natural opening where the nerve exits the spine. Often used for lumbar disc herniations and foraminal stenosis.
- Interlaminar — the endoscope enters from the back, between two laminae. Often used for L5–S1 herniations or central canal decompression.
There are also cervical and thoracic endoscopic techniques, but the lumbar spine is where the evidence base is strongest.
As a DWG-certified spine surgeon practising in Germany, I should be transparent: endoscopic spine surgery is a tool, not a brand of medicine. The question is never "Is endoscopy better?" in the abstract — it is "Is endoscopy the right tool for your specific pathology, in the hands of an experienced surgeon?"
The technology does not perform the surgery. The surgeon does. A skilled microdiscectomy will outperform a poorly executed endoscopic procedure every time.
How Does Endoscopic Spine Surgery Differ From Traditional Surgery?
The main differences are incision size, muscle disruption, anaesthesia, and recovery profile. Endoscopic surgery typically uses a 7–10 mm incision and preserves more of the surrounding muscle and bone. Open or microsurgical approaches use a larger incision (usually 2–4 cm) and involve more soft-tissue retraction.
Here is a practical comparison for a single-level lumbar disc herniation:
Several randomised trials and systematic reviews (including work published in Pain Physician and European Spine Journal) suggest that for properly selected lumbar disc herniations, endoscopic and microsurgical techniques achieve comparable leg-pain relief and functional outcomes at one and two years. The endoscopic group tends to have less early postoperative back pain and faster early recovery, while microsurgery remains the more versatile workhorse.
Who Is a Good Candidate?
You are more likely to be a good candidate if you have:
- A clear, MRI-confirmed lumbar disc herniation that matches your symptoms (usually leg pain greater than back pain, in a specific dermatomal pattern).
- Persistent radicular pain (sciatica) that has not improved after 6–12 weeks of conservative care — physiotherapy, activity modification, appropriate medication, and sometimes a nerve root injection.
- Focal foraminal or lateral recess stenosis at one or two levels.
- A neurological deficit (weakness, numbness) that correlates with imaging.
- No significant spinal instability or deformity at the target level.
Red-flag situations that need urgent in-person assessment, not an online discussion: cauda equina symptoms (saddle numbness, new bladder or bowel changes), rapidly progressing weakness, or suspected infection or tumour. These can be emergencies.
When Is Endoscopic Spine Surgery Not the Right Choice?
This is where honesty matters more than enthusiasm for the technique. Endoscopic surgery is generally less suitable for:
- Significant spinal instability (e.g. high-grade spondylolisthesis) where fusion or stabilisation is needed.
- Severe multilevel central stenosis requiring wide decompression.
- Large, calcified, or migrated disc fragments that are difficult to reach endoscopically.
- Spinal deformity (scoliosis, kyphosis) where alignment correction is the goal.
- Revision surgery with extensive scar tissue, in some cases.
- Tumours or infections requiring broader exposure.
A common mistake I see in online second opinions is patients who have been offered an endoscopic procedure for a problem that really calls for a different operation — or, just as often, for a problem that does not yet need surgery at all. The technology is appealing because it sounds gentle, but the gentlest operation is still the one you do not need.
What Happens Before, During, and After Surgery?
Before
Expect a thorough clinical examination, an up-to-date MRI (usually within the last 6 months), and sometimes flexion-extension X-rays to assess stability. Blood tests, an ECG, and an anaesthetic review are standard. You will be asked to stop certain medications (e.g. anticoagulants) on a defined schedule.
During
A typical lumbar endoscopic discectomy looks like this:
- You are positioned prone (face down) on a special table.
- Anaesthesia is given — sedation with local infiltration, or general, depending on the case and your preference.
- Using live X-ray (fluoroscopy), the surgeon places a guide wire and dilator, then the working cannula.
- The endoscope is inserted, irrigation begins, and the herniated fragment or compressive tissue is removed under continuous video guidance.
- The skin is closed with one or two sutures or skin glue. The incision is usually covered with a small dressing.
Operating time is typically 45–90 minutes for a single level.
After
- First few hours: You rest, eat, and most patients walk within 2–4 hours.
- Day 1–3: Mild incision soreness is normal. Leg pain often improves immediately, though some numbness can take weeks to settle.
- Week 1–2: Light activity, walking, return to desk work for many patients.
- Week 2–6: Gradual reintroduction of physiotherapy and load.
- Week 6–12: Most patients return to sport and heavier work, guided by their surgeon.

What Are the Risks and Realistic Outcomes?
Every spine operation carries risk. For endoscopic lumbar discectomy in experienced hands, published complication rates are generally low, but they are not zero. Reported risks include:
- Recurrent disc herniation (around 3–7% within the first year, similar to microdiscectomy).
- Dural tear (less common than in open surgery, but possible).
- Nerve root irritation or transient numbness/weakness.
- Incomplete decompression requiring conversion to an open procedure.
- Infection (rare with such small incisions, but reported).
- Recurrence of symptoms over time as the disc continues to age.
I never promise a specific outcome to a patient, and I would be cautious of any surgeon who does. What good evidence suggests is that, in well-selected patients, leg-pain relief rates after endoscopic lumbar discectomy are comparable to those after microdiscectomy — broadly in the 80–90% range at one year in published series — but individual results vary with anatomy, duration of symptoms, and overall health.
Why a Second Opinion Is Worth Considering
Spine surgery is a YMYL decision — your mobility and quality of life are at stake. An independent second opinion, whether in person or online, can:
- Confirm that the diagnosis matches your symptoms and imaging.
- Clarify whether surgery is needed now, later, or possibly not at all.
- Compare techniques honestly, including non-endoscopic options.
- Reduce regret. Patients who feel informed tend to recover better psychologically.
I offer online second opinions to patients worldwide, but the point is not who provides the opinion — the point is that you get one. Bring your MRI images (not just the report), a clear symptom timeline, and a list of what you have already tried. A good second opinion should make your situation clearer, not push you toward any particular operation.
FAQ
Is endoscopic spine surgery safer than traditional surgery?
"Safer" is the wrong frame. In well-selected cases and skilled hands, complication rates are comparable to microsurgery, with less early postoperative pain. In the wrong case, smaller incisions do not protect you from a poor outcome.
How long does the surgery itself take?
A single-level lumbar endoscopic discectomy usually takes 45–90 minutes, plus preparation and recovery time.
Will I need general anaesthesia?
Often no. Many endoscopic lumbar procedures can be done under sedation with local anaesthetic, which suits patients with cardiac or respiratory concerns. Your anaesthetist and surgeon will advise.
When can I drive, fly, or return to work?
Most patients drive again within 1–2 weeks, fly short-haul after about 1–2 weeks (longer for long-haul, with movement and hydration), and return to desk work within 1–2 weeks. Physical jobs may require 6–12 weeks.
Does endoscopic surgery work for neck (cervical) problems?
Yes, in selected cases, but the evidence base is smaller and the anatomy less forgiving. Cervical endoscopic surgery should only be done by surgeons with specific advanced training in it.
Can I get a second opinion if surgery has already been scheduled?
Yes, and it is reasonable to do so. A short delay to confirm the plan is almost never harmful (except in true emergencies) and can prevent an avoidable operation.
Conclusion
Endoscopic spine surgery is a genuinely useful, well-evidenced option for specific spinal problems — particularly lumbar disc herniations and selected foraminal stenosis. It offers smaller incisions, less muscle disruption, and a quicker early recovery for the right patient. It is not a universal solution, and it does not turn an unnecessary operation into a good idea.
If you are weighing up surgery, three steps tend to serve patients well:
- Make sure your diagnosis is solid. Imaging must match symptoms; symptoms must match the proposed operation.
- Exhaust reasonable conservative care unless there is a red flag.
- Get an independent second opinion before committing to surgery — online second opinions are a practical option if you cannot easily travel.
Whatever you decide, decide with information, not pressure. Your spine will thank you for the patience.
This article is educational and does not constitute personal medical advice. Please consult a qualified spine specialist for evaluation of your individual condition.