
Last updated: June 8, 2026
Quick Answer
Most people with scoliosis do not need surgery. Surgery is generally considered when the Cobb angle exceeds roughly 45–50 degrees in adolescents with remaining growth, or when adult scoliosis causes progressive curve worsening, intractable pain, or neurological symptoms that fail conservative care. If you have been told you need scoliosis surgery, an independent second opinion before committing to a major deformity operation is reasonable and often valuable.
Key Takeaways
- The Cobb angle is the main number that drives surgical decisions, but it is never the only factor.
- Curves under 25 degrees are usually observed; 25–45 degrees in growing children are often braced; surgery is typically discussed above 45–50 degrees.
- Adult scoliosis is treated differently from adolescent idiopathic scoliosis — pain, function, and progression matter more than degree alone.
- Bracing can slow or stop progression in skeletally immature patients, but it does not reliably reverse curves.
- Major deformity surgery carries real risks; an online second opinion is a low-cost way to confirm the recommendation.
- "Doing nothing" is sometimes the correct medical answer, especially for mild, stable adult curves.
How do I know if my scoliosis curve is serious?
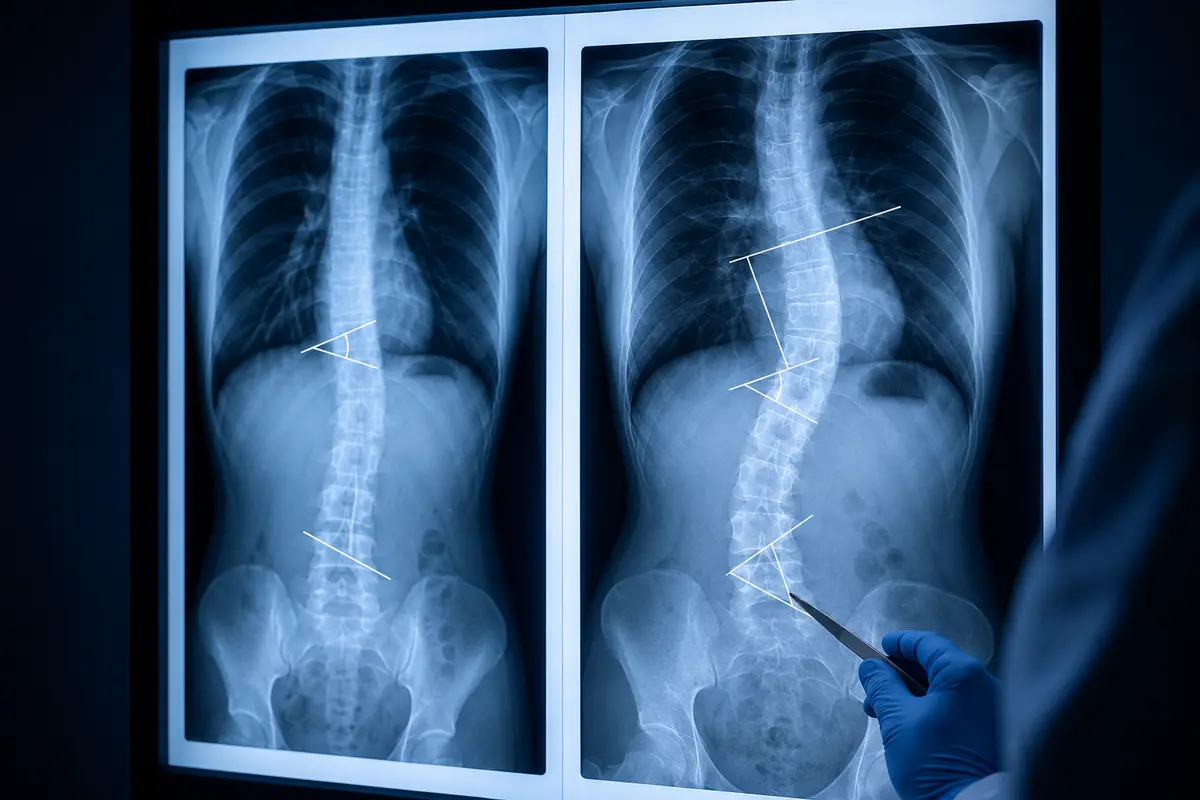
A curve becomes clinically serious when its Cobb angle is large, when it is progressing on serial X-rays, or when it produces symptoms such as pain, breathing limitation, or nerve compression. The Cobb angle is measured on a standing full-spine X-ray between the most tilted vertebrae at the top and bottom of the curve.
As a rough guide used in most international guidelines (including the Scoliosis Research Society and SOSORT recommendations):
Two things make a curve more concerning regardless of degree: documented progression of more than 5 degrees between X-rays, and symptoms such as nerve pain, leg weakness, or reduced lung function.
What degree of curve requires scoliosis surgery?
In adolescents with idiopathic scoliosis, surgery is most commonly recommended at a Cobb angle of around 45–50 degrees or more, particularly if the patient still has growth remaining. In adults, the threshold is less rigid — curves above 50 degrees in the thoracic spine or above 40 degrees in the lumbar spine tend to progress over a lifetime and may eventually warrant surgical correction.
Decision rule I use in consultations:
- Choose surgery seriously if: curve is over 50 degrees and progressing, you have radicular leg pain, sagittal imbalance, or functional decline that conservative care has not improved over 6–12 months.
- Choose to wait if: curve is stable on repeat imaging, pain is manageable, and there is no neurological deficit.
Numbers alone never decide. A flexible 55-degree curve in a healthy teenager is a very different problem from a rigid 45-degree curve in a 70-year-old with osteoporosis.
Can scoliosis get worse without surgery?
Yes, scoliosis can progress without surgery, but progression is not inevitable and depends heavily on age, curve size, and skeletal maturity. Adolescent curves under 30 degrees at skeletal maturity rarely progress significantly in adulthood, while curves over 50 degrees tend to worsen by roughly 0.5–1 degree per year over a lifetime, according to long-term natural history studies.
Risk factors for progression include:
- Remaining skeletal growth (Risser sign 0–2)
- Curve magnitude already above 30 degrees
- Female sex (for adolescent idiopathic scoliosis)
- Thoracic curve location
- Family history of progressive scoliosis
What happens if I don't get scoliosis surgery?
For most people with mild to moderate curves, choosing not to have surgery leads to a normal life expectancy and acceptable function. For severe, progressive curves — especially thoracic curves above 70–80 degrees — long-term consequences can include reduced pulmonary function, chronic back pain, and progressive deformity.
What "no surgery" realistically looks like:
- Periodic monitoring with standing X-rays every 6–24 months
- Physiotherapy, core strengthening, and pain management
- Lifestyle modification (weight, activity, ergonomics)
- Bracing in selected adult cases for symptom relief
The honest answer: avoiding surgery is the right choice for many patients. The wrong choice is avoiding evaluation.
What are alternative treatments to scoliosis surgery?
Non-surgical options for scoliosis include observation, scoliosis-specific physiotherapy (such as Schroth or SEAS methods), bracing, pain management, and targeted injections for adult degenerative cases. None of these reliably "cure" a structural curve, but they can stabilise progression, reduce pain, and improve function.
Evidence-based alternatives by patient group:
- Growing adolescents (25–45 degrees): Rigid TLSO bracing worn 16–23 hours daily. The BrAIST trial (NEJM, 2013) showed bracing significantly reduced progression to the surgical threshold.
- Adults with degenerative scoliosis: Physiotherapy, NSAIDs, epidural or facet injections, lifestyle changes.
- All ages: Scoliosis-specific exercise programmes (PSSE) supervised by trained therapists.
Common mistake: assuming chiropractic manipulation or generic yoga will "correct" a structural curve. There is no high-quality evidence that any manual therapy reduces Cobb angle.
Bracing versus surgery: how do they compare?
Bracing aims to prevent a curve from worsening during growth; surgery aims to correct and stabilise a curve that is already severe or progressive. They serve different purposes at different stages, and they are not interchangeable.
Can teenagers have scoliosis surgery, and how is it different in adults?
Yes, teenagers commonly undergo scoliosis surgery — adolescent idiopathic scoliosis is the most frequent indication worldwide. Adolescent surgery typically achieves greater curve correction with lower complication rates than adult deformity surgery, because younger spines are more flexible and bones heal more reliably.
Key differences:
- Adolescents: Usually posterior spinal fusion with pedicle screws. Goal is correction plus stopping progression. Recovery is faster.
- Adults: Often longer fusions, sometimes combined anterior/posterior approaches, frequently involving the pelvis. Goal shifts toward pain relief, balance, and function rather than maximal cosmetic correction.
- Older adults: Complication rates rise with age, osteoporosis, and comorbidities. Decision-making becomes more nuanced.
Am I too old for scoliosis surgery?
There is no strict age cut-off for scoliosis surgery, but biological age, bone quality, cardiopulmonary fitness, and comorbidities matter far more than the number on your passport. Carefully selected patients in their 70s do undergo successful deformity correction, while some patients in their 50s are not good candidates due to osteoporosis or other risks.
What surgeons actually assess:
- Bone density (DEXA scan)
- Cardiac and pulmonary reserve
- Frailty scores and nutritional status
- Smoking status (a major modifiable risk)
- Realistic functional goals
"Age is a variable, not a verdict. The patient's overall physiological reserve and goals matter more than their date of birth."
How long does scoliosis surgery take, and how painful is recovery?
A standard posterior spinal fusion for adolescent idiopathic scoliosis usually takes 4–6 hours; complex adult deformity surgery can take 6–10 hours or longer. Recovery is genuinely painful in the first 1–2 weeks and gradually improves over 3–6 months, with full bony fusion taking up to 12 months.
A typical recovery timeline:
- Days 1–5: Hospital stay, IV pain control, early mobilisation with physiotherapy.
- Weeks 1–6: Significant fatigue and back discomfort; walking encouraged, no bending or lifting.
- Months 2–6: Gradual return to school, work, light activity. Pain steadily decreases.
- Months 6–12: Return to most sports and full activity once fusion is confirmed.
Pain is well-managed in modern protocols with multimodal analgesia, but I never tell patients it will be easy. Honesty matters.

What are the risks and common complications of scoliosis surgery?
Scoliosis surgery is major surgery with real, well-documented risks. Reported complication rates vary widely by patient age and curve complexity — roughly 5–10% for adolescent idiopathic scoliosis and 20–40% for complex adult deformity surgery in published series.
Recognised complications include:
- Infection (1–5%)
- Blood loss requiring transfusion
- Hardware failure or pseudarthrosis (failed fusion)
- Adjacent segment degeneration over years
- Neurological injury, including, rarely, paralysis (under 1% in most series)
- Persistent pain despite technically successful surgery
- Need for revision surgery (higher in adult deformity)
This is precisely why a second opinion before major deformity surgery is reasonable. If you are facing a long fusion, especially one extending to the pelvis, getting another experienced set of eyes on your imaging is a sensible step — and something I and other surgeons routinely provide online.
How much does scoliosis surgery cost, and will it be covered?
Costs vary enormously by country and healthcare system, so I cannot give a single figure. In most European public healthcare systems (UK NHS, German statutory insurance, etc.), medically indicated scoliosis surgery is covered. In private and self-pay settings worldwide, complex adult deformity surgery is among the more expensive spine procedures because of operative time, implants, and hospital stay.
Practical steps:
- Ask your treating hospital for a written cost estimate, including implants and rehabilitation.
- Confirm coverage in writing with your insurer or national health service before scheduling.
- Factor in time off work and rehabilitation costs.
I do not advise on US billing specifics; speak to your provider directly.
Do I need scoliosis surgery, or should I get a second opinion first?
If surgery has been recommended, an independent second opinion is almost always a good idea — especially for adult deformity surgery, revision surgery, or any procedure involving more than a few fused levels. A second opinion is not about distrusting your surgeon; it is about confirming that a major, irreversible decision is the right one for your specific spine.
Reasonable triggers for seeking a second opinion:
- Fusion of more than 4–5 levels recommended
- Any operation extending to the pelvis
- Disagreement among the clinicians you have already seen
- Borderline Cobb angles (45–55 degrees) where the indication is not clear-cut
- You simply do not feel ready to proceed
An online second opinion lets you upload your imaging and reports for review by an independent spine surgeon without travelling. It is educational, not a replacement for in-person care, but it often clarifies whether surgery is truly necessary now, later, or not at all.
FAQ
Is scoliosis surgery ever an emergency?
Rarely. True emergencies involve acute neurological deterioration, such as progressive leg weakness or loss of bladder control. Most scoliosis surgery is planned weeks or months in advance.
Can exercise alone fix scoliosis?
No. Exercise and scoliosis-specific physiotherapy can improve posture, pain, and function, and may help slow progression, but they do not structurally correct an established curve.
Will I be shorter after fusion surgery?
Most patients actually become slightly taller after correction because the curve is straightened. Spinal flexibility, however, is reduced in the fused area.
How successful is scoliosis surgery?
Adolescent idiopathic scoliosis surgery achieves curve correction of around 50–70% in most series, with high patient satisfaction. Adult deformity outcomes are more variable and depend heavily on patient selection.
Can scoliosis come back after surgery?
The fused portion of the spine cannot re-curve, but adjacent unfused segments can develop new curvature or degeneration over years, sometimes requiring revision surgery.
Should I get an online second opinion before scoliosis surgery?
For any major deformity operation, yes — it is a low-risk, educational step that can either confirm the plan or reveal alternatives worth discussing with your treating team.
Conclusion
Asking "do I need scoliosis surgery?" is one of the most important questions you can ask, and the honest answer is: it depends on your Cobb angle, your age, your symptoms, the rate of progression, and your goals. Most curves do not need surgery. Some clearly do. A meaningful number sit in the grey zone where reasonable surgeons might disagree.
If you are facing a recommendation for spinal fusion, take the following steps:
- Obtain copies of all your imaging and clinical reports.
- Confirm your current Cobb angle and any documented progression.
- Ask your surgeon to explain the specific indication and the alternatives.
- Consider an independent second opinion, particularly for long fusions or adult deformity surgery.
- Make the decision when you feel informed, not rushed.
This article is educational and not a substitute for in-person medical evaluation. If you would like an independent review of your imaging and reports, an online spine second opinion is a straightforward way to get one before committing to surgery.