

Last updated: June 1, 2026
Quick Answer
Degenerative disc disease (DDD) is not truly a "disease" — it is a normal, age-related change in your spinal discs that most adults develop over time. The majority of people with disc degeneration respond well to conservative degenerative disc disease treatment such as structured physiotherapy, activity modification, and pain management, without ever needing surgery. Spinal fusion for back pain alone (without nerve compression or instability) remains controversial, and international guidelines recommend exhausting non-surgical options first. If you have been told you need an operation, seeking an independent second opinion is a reasonable and often valuable step.
Key Takeaways
- DDD is found on MRI in the majority of adults over 40 and is often painless. An abnormal scan does not automatically mean you need treatment.
- Conservative care (physiotherapy, exercise, medication, lifestyle changes) is the first-line degenerative disc disease treatment recommended by NICE and most international spine societies.
- Spinal fusion for axial back pain alone has inconsistent long-term outcomes. Cochrane reviews have not found strong evidence that fusion is superior to structured rehabilitation for this indication.
- Surgery is clearly indicated when there is progressive neurological deficit, significant spinal instability, or failure of prolonged conservative care with matched clinical and imaging findings.
- Physical therapy and core stabilisation have strong evidence supporting their role in reducing pain and improving function.
- Stem cell therapy for disc regeneration is still experimental. No regulatory body has approved it as a standard treatment for DDD as of 2026.
- Lifestyle factors — maintaining a healthy weight, staying active, not smoking — are among the most effective ways to slow disc deterioration.
- An online second opinion from a spine specialist can help you understand whether surgery is truly necessary before committing to an irreversible procedure.
What Exactly Is Degenerative Disc Disease and How Does It Progress?
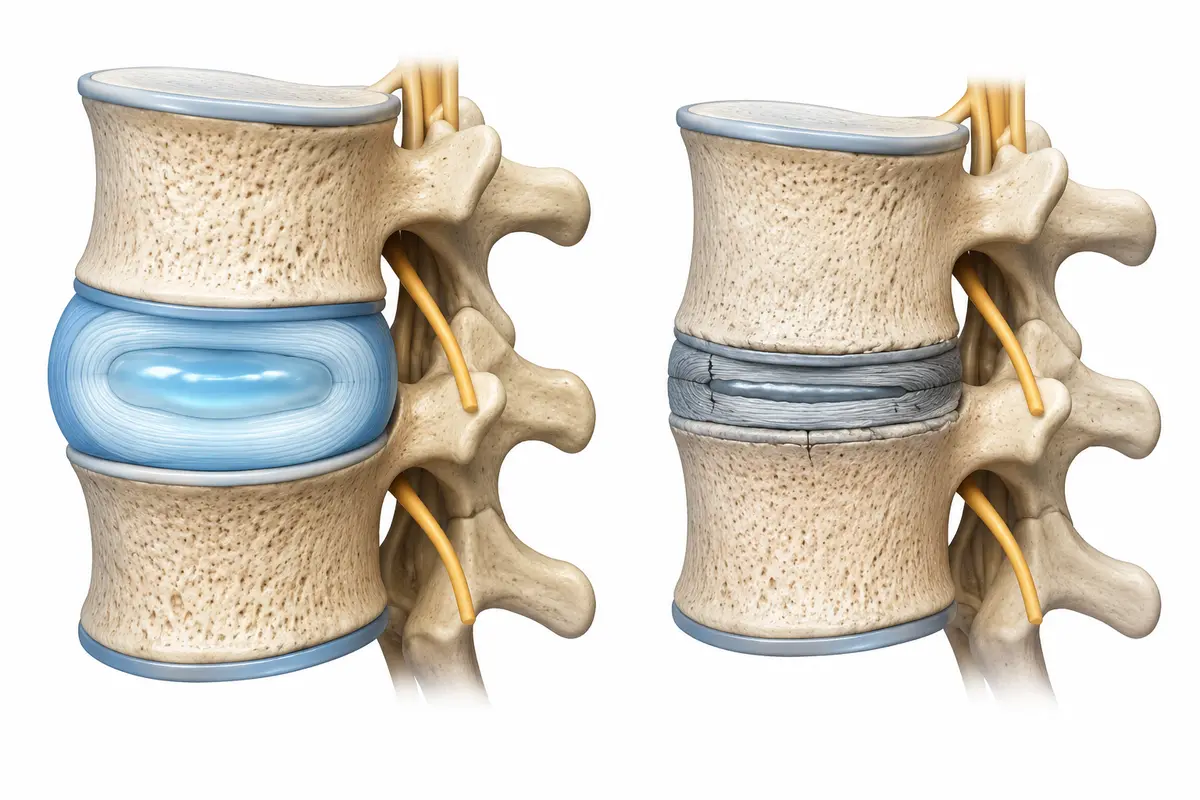
Degenerative disc disease is the gradual wear and tear of the intervertebral discs — the soft, cushion-like structures between your vertebrae. It is a natural part of ageing, not a progressive illness in the way the name suggests.
Here is what happens over time:
- Water loss (desiccation): Discs are about 80% water in youth. With age, they lose hydration and become thinner and less flexible.
- Annular tears: Small tears develop in the tough outer ring (annulus fibrosus). These can sometimes cause localised pain.
- Disc height loss: As the disc flattens, the space between vertebrae narrows, which can affect the facet joints and neural foramina.
- Osteophyte formation: The body responds to instability by forming bone spurs, which may or may not compress nerves.
This process typically begins in the third decade of life. A landmark study published in the American Journal of Neuroradiology (Brinjikji et al., 2015) found disc degeneration on MRI in 37% of 20-year-olds and over 90% of people aged 60 and above — most of whom had no symptoms at all.
Common mistake: Assuming that disc degeneration seen on an MRI is the cause of your pain. In many cases, it is an incidental finding. The clinical picture — your symptoms, examination, and how they match the imaging — matters far more than the scan alone.
How Do I Know If My Back Pain Is From Disc Degeneration?
Discogenic back pain (pain originating from a damaged disc) is typically felt as a deep, aching pain in the lower back that worsens with sitting, bending forward, or lifting. It may improve when lying down or walking.
However, diagnosing discogenic pain with certainty is difficult because:
- Many structures in the spine (facet joints, muscles, sacroiliac joints, ligaments) can produce similar symptoms.
- MRI findings of disc degeneration are extremely common in people without any pain.
- There is no single test that reliably confirms a disc as the pain source.
Decision rule: If your pain is primarily in the back (axial pain) without leg symptoms, and your MRI shows typical age-related changes, the disc degeneration may be coincidental. If you have radiating leg pain, numbness, or weakness that matches a specific nerve root on imaging, the correlation is stronger and more clinically meaningful.
A thorough clinical assessment by a spine specialist — correlating your history, physical examination, and imaging — is essential before attributing pain to disc degeneration.
Am I Too Young or Too Old to Have Degenerative Disc Problems?
No one is truly "too young" or "too old." Disc degeneration can begin in adolescence and is nearly universal by old age. Genetics play a significant role — twin studies have shown that hereditary factors account for a large proportion of disc degeneration, sometimes more than mechanical loading or occupation.
For younger patients (20s–30s): Early disc changes are common and usually do not require treatment. Heavy manual labour, smoking, and obesity can accelerate the process. If you are young and experiencing significant symptoms, a thorough evaluation is warranted, but surgery is rarely the first answer.
For older patients (70s and beyond): Age alone does not disqualify you from treatment, but surgical risk increases with comorbidities. Conservative management is often preferred, and many older adults find that their disc-related pain actually diminishes over time as the spine naturally stiffens and stabilises.
What Are the Best Non-Surgical Treatments for Disc Degeneration?
For most people, conservative management is the recommended first-line degenerative disc disease treatment. The goal is to reduce pain, improve function, and help you stay active.
Evidence-based non-surgical options include:
Choose conservative care if: Your pain is primarily axial (in the back), you have no progressive neurological symptoms, and you have not yet completed a structured rehabilitation programme of at least 3–6 months.
Can Physical Therapy Actually Help With Disc Degeneration?
Yes. Physiotherapy is one of the most consistently supported treatments for back pain associated with disc degeneration. It won't reverse the structural changes in your disc, but it can significantly reduce pain and improve your ability to function.
The key components of an effective programme include:
- Core stabilisation exercises — strengthening the deep muscles (transversus abdominis, multifidus) that support the spine
- Graded activity and aerobic conditioning — walking, swimming, or cycling to improve overall fitness and reduce pain sensitivity
- Flexibility work — gentle stretching of the hip flexors, hamstrings, and thoracic spine
- Education — understanding that movement is safe and beneficial, even when it causes some discomfort
NICE guidelines for low back pain and sciatica recommend exercise and physiotherapy as core treatments. Cochrane reviews on exercise therapy for chronic low back pain have consistently found that exercise reduces pain and improves function compared to no treatment or usual care.
Edge case: If physiotherapy consistently worsens your symptoms despite proper technique and gradual progression, discuss this with your treating clinician. It may indicate an alternative pain generator or the need for further investigation.
What Exercises Should I Avoid If I Have Degenerative Disc Disease?
There are no universally banned exercises, but certain movements may aggravate symptoms in some people with disc-related pain.
Exercises to approach with caution:
- Heavy deadlifts and squats with poor form — these increase compressive load on the discs significantly
- Repeated trunk flexion (e.g., sit-ups, toe touches) — may irritate an already sensitised disc
- High-impact activities (running on hard surfaces, jumping) — can worsen symptoms in acute flare-ups
- Prolonged static positions — sitting for hours without breaks
What to do instead:
- Focus on neutral-spine exercises (bird-dogs, planks, bridges)
- Swim or walk regularly
- Use pain as a guide — mild discomfort during exercise is often acceptable, but sharp or worsening pain is a signal to modify
The goal is to stay active, not to avoid movement. Deconditioning (becoming less fit due to inactivity) is one of the biggest risk factors for chronic back pain.
How Do Conservative Treatments Compare to Surgical Options?
For axial back pain without nerve compression or instability, structured conservative care performs comparably to — and sometimes better than — surgery in long-term studies.
Key evidence:
- The Swedish Lumbar Spine Study (Fritzell et al., 2001) found that fusion was superior to "usual care" for chronic low back pain, but "usual care" in that study was not a structured rehabilitation programme.
- A subsequent trial by Brox et al. (2003, 2006) compared fusion to a structured cognitive-behavioural and exercise programme and found no significant difference in outcomes at long-term follow-up.
- Cochrane reviews have concluded that there is insufficient evidence to recommend fusion over comprehensive rehabilitation for chronic low back pain.
When surgery is more clearly indicated:
- Progressive neurological deficit (worsening weakness or loss of bladder/bowel control)
- Significant structural instability (e.g., spondylolisthesis with motion)
- Radiculopathy (leg pain from nerve compression) that has failed prolonged conservative care
- Matched clinical and imaging findings confirming the pain source
Common mistake: Agreeing to fusion based solely on MRI findings of disc degeneration without a thorough trial of conservative management. This is where a second opinion can be particularly valuable.
What Are the Risks of Spinal Fusion Surgery?
Spinal fusion is a major operation. While it can be the right choice for specific indications, patients should understand the risks before proceeding.
Potential risks include:
- Adjacent segment disease — the levels above and below the fusion may degenerate faster due to altered biomechanics (reported in up to 25–30% of patients over 10 years in some series)
- Non-union (pseudarthrosis) — the bones may fail to fuse, potentially requiring revision surgery
- Infection — surgical site infection rates vary but are typically 1–5%
- Nerve damage — rare but possible, especially with revision procedures
- Hardware failure — screws or rods can loosen or break
- Persistent pain — fusion does not guarantee pain relief, particularly for axial back pain
- General surgical risks — blood clots, anaesthesia complications, wound healing problems
In my practice, I see patients every week who were recommended fusion for back pain alone, without having tried structured physiotherapy or multidisciplinary rehabilitation. I strongly encourage anyone in this situation to seek an independent second opinion before committing to an irreversible procedure.
Can Stem Cell Therapy Really Repair Damaged Discs?
As of 2026, stem cell therapy for disc regeneration remains experimental. There is early-phase research showing some promise, but no large, randomised controlled trials have demonstrated reliable disc repair or long-term pain relief.
What the evidence shows:
- Small pilot studies have injected mesenchymal stem cells into degenerated discs with some short-term improvements in pain scores.
- No therapy has been shown to reliably restore disc height or hydration in humans.
- No major regulatory body (EMA, FDA, NICE) has approved stem cell injections as a standard treatment for DDD.
Caution: Many private clinics worldwide market stem cell treatments for disc disease at significant cost, often without robust evidence. If you are considering this, ask for published trial data, not just testimonials. Be wary of clinics that make promises of disc regeneration or "cures."

Which Specialists Should I See for Disc Disease?
Start with your general practitioner or family doctor, who can assess your symptoms, arrange imaging if needed, and refer you appropriately.
Relevant specialists include:
- Physiotherapist — for exercise-based management (often the most important member of the team)
- Spine surgeon (orthopaedic or neurosurgeon) — for evaluation if surgery is being considered
- Pain medicine specialist — for injection therapies or medication management
- Rheumatologist — if an inflammatory cause is suspected
- Psychologist or pain psychologist — for chronic pain management, particularly if pain is affecting mood, sleep, or daily life
Decision rule: See a spine surgeon if you have progressive neurological symptoms, if conservative care has failed after 3–6 months, or if you want a specialist opinion on whether your imaging findings are clinically relevant. You do not need to see a surgeon first — in fact, starting with physiotherapy is often more efficient.
What Lifestyle Changes Can Slow Down Disc Deterioration?
You cannot stop disc ageing entirely, but you can slow its progression and reduce the likelihood of symptoms.
- Stay physically active — regular moderate exercise maintains disc nutrition (discs rely on movement for nutrient exchange, as they have limited blood supply)
- Maintain a healthy weight — excess body weight increases compressive forces on the lumbar spine
- Stop smoking — smoking impairs blood flow to the disc and accelerates degeneration. This is one of the most modifiable risk factors.
- Manage your posture and ergonomics — especially if you have a sedentary job. Stand regularly, use a supportive chair, and vary your position throughout the day.
- Stay hydrated and eat well — while no specific diet has been proven to reverse disc degeneration, an anti-inflammatory diet rich in omega-3 fatty acids, vegetables, and lean protein supports general musculoskeletal health.
Are There Any Natural Supplements That Help With Disc Health?
There is limited high-quality evidence for supplements specifically targeting disc health. Some supplements have general anti-inflammatory or joint-supporting properties, but none have been proven to regenerate or repair spinal discs.
Supplements sometimes discussed:
- Glucosamine and chondroitin — widely used for joint health; evidence for spinal disc benefit is weak
- Omega-3 fatty acids (fish oil) — may have mild anti-inflammatory effects
- Vitamin D — deficiency is associated with musculoskeletal pain; supplementation is reasonable if levels are low
- Turmeric/curcumin — some anti-inflammatory properties in laboratory studies; clinical evidence for back pain is limited
- Collagen peptides — marketed for disc and joint health; evidence is preliminary
My advice: Supplements should not replace physiotherapy, exercise, or medical treatment. If you choose to use them, discuss this with your doctor, particularly if you take other medications. Do not rely on supplements as a primary degenerative disc disease treatment.
How Much Does Treatment Cost Without Insurance?
Treatment costs vary enormously depending on your country, the type of treatment, and the healthcare system.
These are broad estimates and will differ based on location. In many European countries, public healthcare systems cover most or all of these costs. For patients travelling internationally for treatment, it is worth requesting a detailed cost breakdown in advance.
An online second opinion — typically costing a fraction of surgery — can help you determine whether an expensive procedure is truly necessary. I offer this service for patients worldwide and find that a significant proportion of patients referred for surgery benefit from continued conservative management instead.
Frequently Asked Questions
Is degenerative disc disease a serious condition?
In most cases, no. DDD is a normal part of ageing and does not usually lead to disability. The term "disease" is misleading. Most people with disc degeneration on MRI have no symptoms or manage well with conservative care.
Can degenerative disc disease be cured?
There is no cure that reverses disc ageing. However, symptoms can be effectively managed in the vast majority of patients through exercise, lifestyle changes, and appropriate medical treatment. Many people achieve significant pain reduction or near-complete symptom relief without surgery.
How long should I try conservative treatment before considering surgery?
International guidelines generally recommend at least 3–6 months of structured conservative care, including a supervised exercise programme, before considering surgery for back pain. Exceptions include progressive neurological deficit or cauda equina syndrome, which require urgent evaluation.
Will my disc degeneration get worse over time?
The structural changes will likely progress slowly with age, but this does not mean your pain will worsen. Many patients find that symptoms improve or stabilise over time, particularly with regular exercise and healthy lifestyle habits.
Is an online second opinion reliable?
An online second opinion from a qualified spine specialist can provide valuable guidance based on your imaging, reports, and clinical history. It is not a replacement for an in-person examination, but it can help you understand your diagnosis, evaluate whether surgery is appropriate, and identify alternative treatment options.
Should I avoid all physical activity if I have DDD?
Absolutely not. Staying active is one of the best things you can do. Prolonged rest and inactivity worsen back pain and lead to deconditioning. Focus on low-impact activities and exercises that strengthen your core without excessive spinal loading.
Conclusion
Degenerative disc disease is one of the most common findings in spine imaging — and one of the most commonly over-treated. The name itself causes unnecessary fear. In reality, disc degeneration is a normal part of ageing that most people experience without significant problems.
If you are dealing with back pain attributed to DDD, here are your next steps:
- Commit to a structured physiotherapy programme for at least 3–6 months before considering surgery.
- Address modifiable risk factors — stop smoking, maintain a healthy weight, stay active.
- Understand your imaging — an MRI showing disc degeneration does not automatically mean you need an operation.
- If surgery has been recommended, seek an independent second opinion. This is especially important if the recommendation is for spinal fusion based on axial back pain alone.
- Be cautious of unproven treatments — stem cell injections and expensive supplements are not yet supported by strong evidence.
As a spine surgeon, I operate when surgery is clearly indicated and likely to help. But I also believe that one of the most important things I can do is help patients avoid unnecessary surgery. If you have been told you need an operation for degenerative disc disease and you are unsure, I am available for online second opinions and would be glad to review your case.
Your spine is more resilient than you might think. With the right approach, most people with disc degeneration live full, active lives.