

Last updated: June 13, 2026
Quick Answer
Cauda equina syndrome (CES) is a rare but serious spinal emergency in which the bundle of nerves at the base of the spinal cord becomes severely compressed. The cauda equina syndrome symptoms you must never ignore are: new difficulty passing urine or loss of bladder control, numbness in the saddle area (groin, inner thighs, buttocks), faecal incontinence, and rapidly worsening leg weakness. If any of these appear, go to A&E immediately — surgical decompression is generally recommended within 24 to 48 hours of symptom onset to give the best chance of recovery.
Key Takeaways
- CES is uncommon but a true neurosurgical emergency; delay can cause permanent loss of bladder, bowel and sexual function.
- The most specific cauda equina syndrome symptoms are saddle numbness, urinary retention or incontinence, and bowel dysfunction — not back pain alone.
- A herniated lumbar disc is the most common cause, but tumours, infection, trauma and spinal stenosis can also trigger CES.
- Urgent MRI is the diagnostic test of choice; do not wait for a routine scan if red flags are present.
- Surgery within 24 to 48 hours of red-flag onset is associated with better outcomes in most published series.
- Young, active adults can absolutely develop CES — it is not an "older person's" condition.
- If you have been told you need spinal surgery for a non-emergency disc problem, a second opinion is reasonable. If you have CES red flags, skip the second opinion and go straight to hospital.
What exactly is cauda equina syndrome and how serious is it?
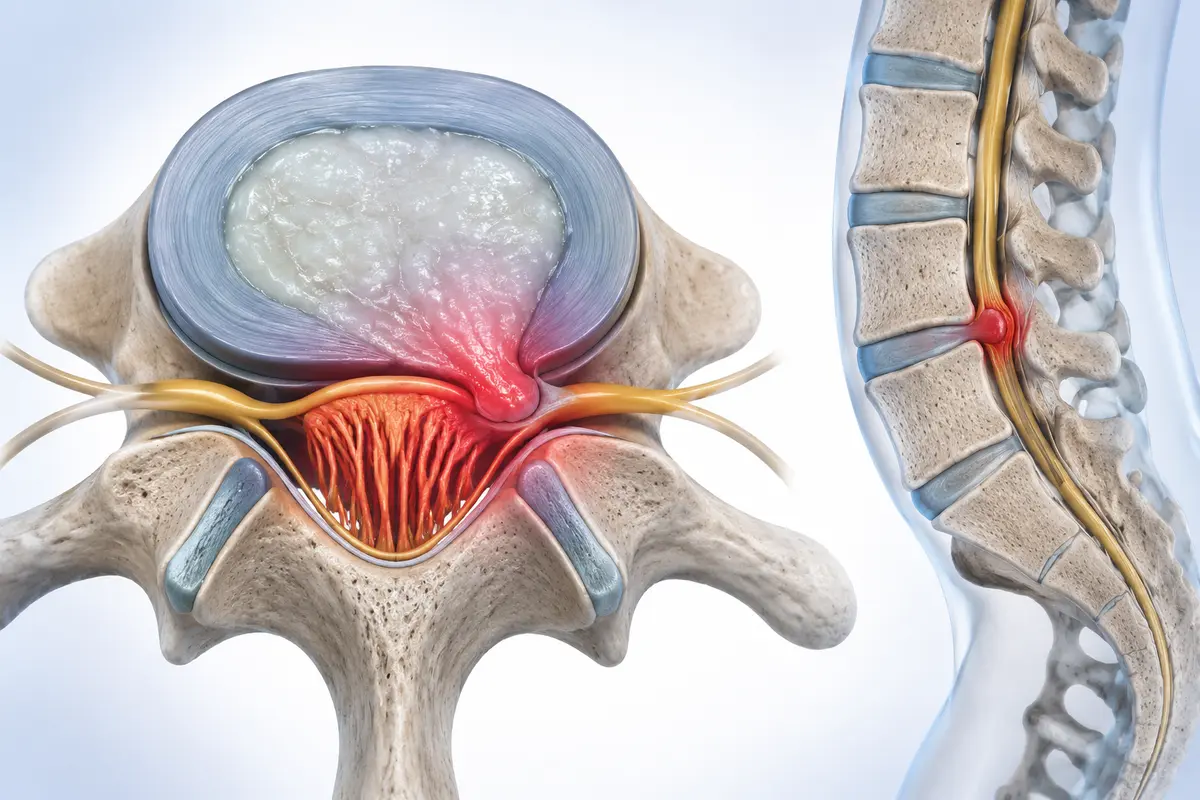
Cauda equina syndrome is the compression of the cauda equina — Latin for "horse's tail" — the bundle of lumbar and sacral nerve roots that hangs below the end of the spinal cord (around the L1-L2 level). These nerves control sensation in the saddle area, leg strength below the knee, and the bladder, bowel and sexual organs.
It is serious. Untreated or delayed CES can leave a person with permanent incontinence, sexual dysfunction, chronic neuropathic pain and leg weakness. Estimates of incidence vary in the literature, but CES is generally cited as affecting roughly 1 to 3 people per 100,000 per year. Rare, but devastating when missed.
As a spine surgeon, I tell patients this plainly: most back pain is not CES, and most disc herniations do not cause CES. But when the red flags appear, the clock starts.
How do I know if my back pain is cauda equina or just normal pain?
Ordinary mechanical back pain, even severe sciatica, does not usually affect bladder, bowel or saddle sensation. CES is distinguished by neurological symptoms below the waist, not by pain intensity.
Use this quick contrast:
Pain alone — even severe pain — is not the deciding factor. It's the loss of function in the areas the cauda equina controls.
What are the early warning signs I should never ignore?
These are the cauda equina syndrome symptoms that should send you to A&E, not to a GP appointment next week:
- Saddle anaesthesia — numbness or pins-and-needles in the groin, inner thighs, buttocks, or around the anus. Test it: does toilet paper feel normal?
- Urinary changes — difficulty starting urination, a weak stream, not feeling the bladder fill, or new incontinence.
- Bowel changes — incontinence, or no longer feeling the urge to pass stool.
- Sexual dysfunction — new genital numbness or sudden erectile/orgasmic changes alongside back pain.
- Bilateral leg symptoms — weakness, numbness or sciatica affecting both legs at once.
- Rapidly progressing weakness — foot drop, difficulty climbing stairs, or legs giving way.
A useful clinical pearl: if you can no longer feel the toilet seat, or you cannot tell when you are urinating, that is a red flag until proven otherwise.
CES is one of the few situations in spine care where waiting and watching is the wrong answer. If you're unsure, be unsure in a hospital, not at home.
Can cauda equina syndrome cause permanent damage if not treated quickly?
Yes. Nerve roots that are compressed for too long lose function, and that loss can be permanent. The literature is consistent that earlier decompression is associated with better recovery of bladder, bowel and sexual function, though no surgeon can guarantee a full recovery even with prompt surgery.
The clinical distinction often made is between:
- CES-S (suspected/incomplete): red flags present but bladder function partially preserved.
- CES-I (incomplete): altered urinary sensation, difficulty voiding, but not yet in painless retention.
- CES-R (retention): painless urinary retention with overflow incontinence — the most advanced stage, with the poorest recovery prognosis.
The practical message: catching CES before it progresses to painless retention matters enormously. This is why the 24-to-48-hour window from red-flag onset is taken so seriously by spine units worldwide.
What medical tests diagnose cauda equina syndrome?
The diagnostic standard is an urgent MRI of the lumbosacral spine, ideally within hours of presentation. CT can be used if MRI is contraindicated (for example, certain pacemakers), but it's less sensitive for nerve compression.
A proper CES work-up typically includes:
- Focused neurological exam: saddle sensation, anal tone, reflexes, leg power.
- Post-void bladder ultrasound or catheterisation to measure residual urine — a large residual volume is a strong red flag.
- Urgent MRI of the whole lumbar spine (a limited scan can miss higher compression).
- Blood tests if infection (discitis, epidural abscess) is suspected.
If an emergency department says "we'll book an outpatient MRI for next week" despite clear red flags, that is not appropriate care. Politely insist, or seek another hospital.
Who is most likely to get cauda equina syndrome, and are athletes at higher risk?
CES can occur at any age, but it most commonly affects adults aged 30 to 60 — the same age range in which large lumbar disc herniations are most common. Men and women are affected at roughly similar rates.
Risk factors include:
- A pre-existing large central lumbar disc herniation (most common cause).
- Severe lumbar spinal stenosis.
- Spinal trauma (falls, road traffic collisions).
- Spinal tumours (primary or metastatic).
- Spinal infection (epidural abscess, discitis).
- Recent spinal surgery (rare post-operative complication).
- Bleeding disorders or anticoagulant therapy (epidural haematoma).
Athletes in heavy-loading sports — weightlifters, rugby players, gymnasts — have a higher rate of disc herniation in general, so they sit in a slightly higher-risk pool, but CES itself remains rare. Manual labourers and anyone with a history of significant disc disease should know the red flags by heart.
Can young people get cauda equina syndrome?
Yes. I have seen patients in their twenties and even late teens with CES, usually from a large acute disc herniation after a lifting injury or sports event. The "young, fit, can't be serious" assumption is one of the most dangerous mistakes — both for patients and for clinicians who under-triage them.
If you are 25, otherwise healthy, and you wake up with numb genitals and can't feel yourself urinating, you have a spinal emergency until imaging proves otherwise.
What emergency symptoms mean I need to go to the hospital immediately?
Go to A&E (Accident & Emergency / Emergency Department) now, not tomorrow, if you have back or leg pain plus any of:
- New difficulty passing urine, or new urinary incontinence.
- New numbness in the saddle area (groin, inner thighs, buttocks, anus).
- New faecal incontinence or loss of the urge to defecate.
- Sudden new sexual numbness or dysfunction.
- New weakness in both legs.
- Rapidly worsening leg weakness on one side.
Take someone with you if possible, bring a list of medications, and clearly state on arrival: "I have back pain with possible cauda equina red flags." Those exact words trigger a recognised triage pathway in most countries.

What are the most common mistakes people make when experiencing symptoms?
From the cases I review for second opinions, the recurring mistakes are:
- Waiting to "see if it settles overnight." Saddle numbness and urinary changes do not need observation; they need imaging.
- Booking a GP appointment instead of going to A&E. GPs cannot order same-day emergency MRI in most systems.
- Assuming strong painkillers explain the numbness. Opioids cause constipation, not saddle anaesthesia.
- Stopping fluids to avoid leakage. This masks retention and worsens the picture.
- Going to a chiropractor or physiotherapist with red flags. Manipulation in undiagnosed CES can be harmful.
- Refusing catheterisation in A&E. A bladder scan and catheter give critical diagnostic information.
How much does surgery for cauda equina syndrome typically cost, and how long is recovery?
Costs vary enormously by country and healthcare system, so I will not quote figures that mislead an international reader. In the UK, CES surgery is provided urgently through the NHS at no cost to the patient. In Germany, statutory and private insurance cover emergency spinal decompression. In countries without universal coverage, emergency departments are still legally obliged to treat life- and function-threatening emergencies — get to hospital first, sort out paperwork after.
Recovery has two timelines:
- Surgical recovery: most patients are mobilising within 1 to 3 days post-op and discharged within a week after a standard lumbar microdiscectomy or decompression. Wound healing takes around 2 to 6 weeks.
- Neurological recovery: this is the longer and less predictable part. Bladder and bowel recovery can continue for 12 to 24 months. Some patients regain near-normal function; others have lasting deficits. Earlier surgery, less severe pre-op deficit, and younger age generally predict better outcomes, though no outcome is guaranteed.
Rehabilitation typically involves pelvic floor physiotherapy, bladder retraining, and gradual return to activity guided by a spine team.
When a second opinion makes sense — and when it doesn't
I provide online spine second opinions for patients worldwide, and I want to be honest about where that fits in CES:
- If you have active CES red flags right now: do not seek a second opinion. Go to A&E. Hours matter.
- If you have been diagnosed with CES, had emergency surgery, and are now being advised on further procedures (fusion, revision): a second opinion is very reasonable. The emergency is over; the long-term plan deserves scrutiny.
- If you have a large disc herniation without CES and have been told you need surgery: a second opinion is often valuable. Many of these cases have non-surgical options.
An independent review can clarify whether a recommended operation is truly necessary, what the alternatives are, and what recovery realistically looks like — but it is never a substitute for emergency care when red flags are present.
FAQ
Is cauda equina syndrome always caused by a slipped disc?
No. A large central lumbar disc herniation is the most common cause, but CES can also result from tumours, spinal infection, trauma, severe stenosis, or epidural haematoma. The cause is identified on MRI.
Can cauda equina syndrome resolve on its own?
No. CES is caused by mechanical compression of nerve roots. The compression must be relieved, almost always surgically. Waiting risks permanent damage.
How quickly does surgery need to happen?
Most spine units aim for decompression within 24 to 48 hours of red-flag onset, and as soon as feasible within that window. The exact timing is debated in the literature, but earlier is generally better.
Will I definitely recover bladder function after surgery?
Not guaranteed. Recovery depends on how severe and how prolonged the compression was before surgery, your age, and the underlying cause. Many patients recover substantially; some have lasting changes.
Can CES come back after successful surgery?
Recurrence is uncommon but possible if a new disc herniation or other compressive lesion develops. Any return of red-flag symptoms after surgery should be treated as an emergency.
Should I get an MRI just to "rule out" CES if I have bad back pain but no red flags?
Not routinely. Imaging is guided by symptoms. In the absence of red flags, most back pain improves with conservative care, and early MRI often shows incidental findings that confuse rather than help.
Conclusion
Cauda equina syndrome is rare, but it is one of the few spinal conditions where hours genuinely change lives. The cauda equina syndrome symptoms that matter most are not back pain itself but the new neurological signs below the waist: saddle numbness, bladder and bowel changes, sexual numbness, bilateral leg weakness. If any of those appear, the next step is A&E — not a GP, not a physiotherapist, not "let's see how it is tomorrow."
For everything else in spine care — chronic back pain, sciatica, disc herniations without red flags, fusion recommendations — there is usually time to think, to ask questions, and to seek an independent second opinion before consenting to surgery. That measured approach is exactly what I encourage in my second-opinion practice.
Know the red flags. Share this with someone who has back pain. And if your gut says something is seriously wrong, trust it and get scanned.
This article is educational and does not constitute personal medical advice. If you have symptoms of cauda equina syndrome, seek emergency in-person assessment immediately.