
Last updated: June 10, 2026
Quick Answer
A bulging disc is a broad, even outward swelling of a spinal disc, while a herniated disc is a focal tear where the inner gel pushes through the outer wall. The terms are often used interchangeably, but they describe different things on MRI. For most people, the distinction matters less than the symptoms: both can be silent in healthy adults, and both usually improve without surgery.
Key Takeaways
- A bulging disc affects a wider area of the disc; a herniated disc is a focal, often smaller, but more aggressive-looking change.
- Disc bulges and herniations are extremely common in pain-free people, especially after age 40.
- Pain severity does not reliably match what you see on MRI.
- Most disc problems improve within 6 to 12 weeks with conservative care.
- Red flags (loss of bladder/bowel control, progressive weakness, saddle numbness) require urgent in-person assessment.
- Surgery helps a specific subset of patients, not the majority.
- A second opinion before spine surgery is reasonable and widely encouraged.
What exactly is a bulging disc, and how is it different from a herniated disc?
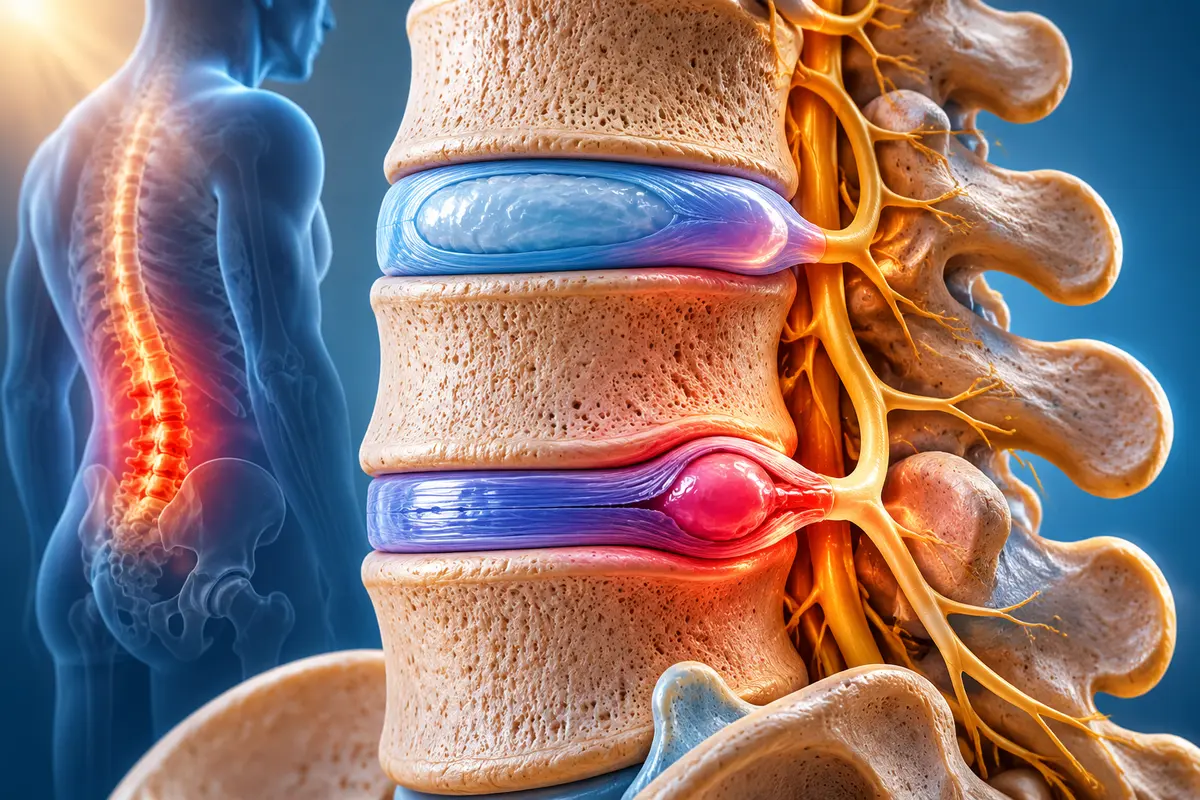
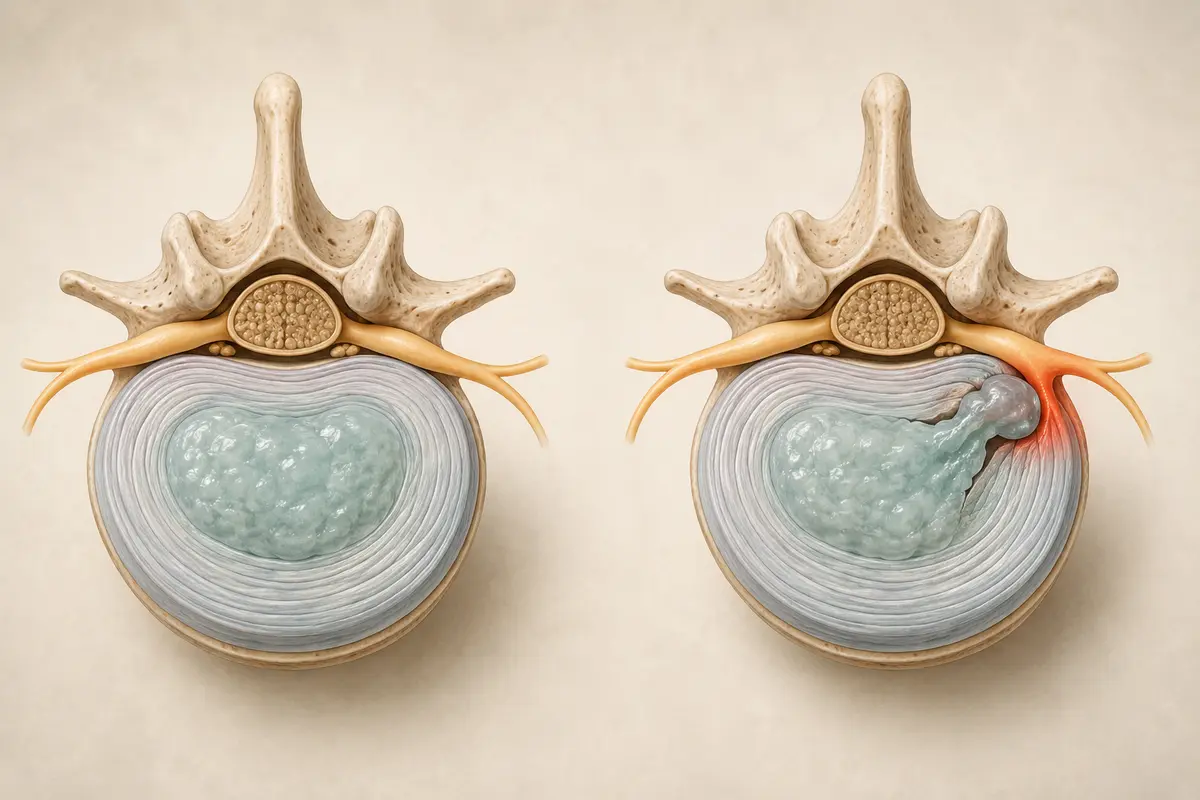
A bulging disc is when an intervertebral disc extends evenly beyond its normal boundary, like a tyre sagging under weight. A herniated disc is when the soft inner core (nucleus pulposus) breaks through a tear in the tougher outer ring (annulus fibrosus). In short: bulging is broad and contained; herniated is focal and often involves a rupture.
Radiologists generally use more precise terms from the North American Spine Society (NASS) lexicon:
- Bulge: disc extends beyond the vertebral edge over more than 25% of its circumference.
- Protrusion: focal extension under 25%, where the base is wider than the tip.
- Extrusion: the displaced material is narrower at the base than at the tip (a true herniation).
- Sequestration: a fragment has broken off entirely.
In everyday speech and even in clinic letters, "herniated disc," "slipped disc," "prolapsed disc," and "ruptured disc" are often used interchangeably. They're not always wrong, just imprecise.
Can a bulging disc turn into a herniated disc?
Yes, it can, but it often doesn't. A bulge reflects general wear in the disc wall. If that wall tears, inner material can push through and become a herniation. Many bulges remain stable for years or decades without ever progressing.
What raises the risk of progression:
- Repeated heavy lifting with poor technique
- Sudden axial loading (e.g., a fall, a car accident)
- Smoking, which reduces disc nutrition
- Genetic predisposition to disc degeneration
What I tell my second-opinion patients: a bulging disc on MRI is not a ticking clock. It's a snapshot of normal age-related change in most adults.
Which condition is more serious or more painful?
Neither is automatically worse. Pain depends on whether the disc material irritates a nerve root, not on the label. A small herniation pressing directly on a nerve can be agonising. A large bulge that touches no nerve may cause nothing at all.
A useful decision rule: symptoms matter more than imaging. Sciatica down the leg below the knee, weakness in a specific muscle group, or numbness in a defined skin area suggests true nerve involvement. Generalised back stiffness without leg symptoms is rarely a surgical problem.
"I've reviewed MRIs that looked alarming for patients who felt fine, and 'mild' scans for patients in genuine distress. The picture is only part of the story."
What symptoms tell me which one I have?
You usually can't tell from symptoms alone, and that's an important point. Both conditions can cause:
- Low back or neck pain
- Pain radiating into an arm or leg (radiculopathy)
- Numbness or tingling along a nerve path
- Weakness in specific muscles
- Pain worse with sitting, coughing, or bending forward
Herniations more often cause sharp, focal leg or arm pain because they tend to press directly on a nerve root. Bulges more often cause diffuse, achy back symptoms. But there's significant overlap, and only imaging combined with a clinical exam can clarify the picture.
Red flags that need urgent in-person care:
- Loss of bladder or bowel control
- Numbness in the groin or inner thighs (saddle anaesthesia)
- Rapidly worsening leg weakness
- Fever with back pain
- Unexplained weight loss
These can signal cauda equina syndrome, infection, or other serious conditions, and are not something to manage online.
How do doctors diagnose the difference?
Diagnosis combines history, physical exam, and imaging — usually MRI. Plain X-rays show bones but not discs. CT can show discs but exposes you to radiation and is less detailed than MRI for soft tissue.
A proper workup includes:
- History: when symptoms started, what aggravates them, red flag screen.
- Neurological exam: reflexes, muscle strength, sensation, straight-leg raise.
- MRI: typically the gold standard, ordered when symptoms persist beyond 6 weeks or when red flags appear.
- Correlation: the imaging must match the symptoms. An L5-S1 herniation should produce L5-S1 symptoms.
This last step is where many patients get misled. A finding on MRI is only meaningful if it explains your symptoms. A landmark study by Brinjikji and colleagues (published in the American Journal of Neuroradiology, 2015) found disc bulges in 30% of pain-free 20-year-olds and over 80% of pain-free 80-year-olds. Disc degeneration showed similar patterns. In other words: MRI findings are often incidental.
Comparison at a glance
Who is most likely to develop a bulging or herniated disc?
Disc changes are part of normal ageing, but several factors raise the risk:
- Age 30 to 50 for symptomatic herniations; bulges become near-universal after 60.
- Occupational loading: heavy lifting, prolonged sitting, vibration (e.g., long-haul driving).
- Smoking, which impairs disc nutrition.
- Higher body weight, which increases axial load.
- Genetics: family history is one of the strongest predictors.
- Sedentary lifestyle combined with sudden bursts of heavy activity.
Athletes can also develop disc problems, but regular moderate exercise is protective overall.
What treatments work best for each?
Treatment overlaps almost entirely. The first-line approach for both is conservative care, and most international guidelines (including NICE NG59 for low back pain and sciatica) recommend the same stepwise pathway:
- Education and reassurance — knowing the condition usually improves is itself therapeutic.
- Stay active — bed rest beyond 1 to 2 days is counterproductive.
- Physiotherapy — graded exercise, often the single most effective intervention.
- Pain control — paracetamol, short courses of NSAIDs, sometimes neuropathic agents for nerve pain.
- Manual therapy — can help short-term.
- Epidural steroid injections — considered for persistent radicular pain.
- Surgery — reserved for failed conservative care with matching imaging, or for red flags.
A Cochrane review on surgery for lumbar disc herniation found that discectomy can speed up recovery from sciatica, but at 1 to 2 years, surgical and non-surgical patients often reach similar outcomes. That's a powerful argument for patience, not panic.
Can I exercise with a bulging or herniated disc?
Yes, and you generally should. Movement is medicine for most disc problems. The old advice of bed rest has been abandoned in modern guidelines.
Safer choices early on:
- Walking
- Swimming or aquatic exercise
- Stationary cycling
- Gentle core work (e.g., dead bugs, bird-dogs)
- Guided physiotherapy
Things to be cautious with while symptoms are acute:
- Heavy deadlifts and squats
- Repeated end-range forward bending under load
- High-impact sports until pain settles
If a specific movement reliably worsens leg pain or weakness, stop and get assessed. Discomfort that fades within minutes is usually fine.
How much does treatment cost?
Costs vary enormously by country, health system, and provider. Rather than quote figures that won't apply internationally, I'd frame it this way:
- Conservative care (physiotherapy, medication, time) is almost always cheaper than surgery, often by an order of magnitude.
- Imaging (MRI) costs differ widely by region and whether ordered privately or through a public system.
- Surgery is the most expensive option and carries the highest risk profile.
Because costs are so variable, the more useful question is: what gives the best risk-adjusted outcome for your specific situation? That's where a second opinion can be valuable — not to save money, but to make sure money and risk are spent on the right intervention.

What are the long-term risks of ignoring symptoms?
Most uncomplicated disc problems do not cause long-term damage if managed sensibly. However, ignoring true warning signs can be serious.
- Persistent severe nerve compression can lead to lasting weakness or numbness.
- Cauda equina syndrome is a surgical emergency; delay risks permanent bladder, bowel, and sexual dysfunction.
- Chronic pain syndromes can develop when acute pain is poorly managed and fear of movement sets in.
"Ignoring" is different from "watching and waiting under guidance." Active monitoring with a clinician is reasonable; pretending symptoms don't exist is not.
Common mistakes people make with disc problems
From the second opinions I review, the most frequent missteps are:
- Treating the MRI, not the patient. Surgery aimed at a "scary-looking" scan without matching symptoms often disappoints.
- Bed rest for weeks. Worsens stiffness, deconditioning, and fear-avoidance.
- Jumping to surgery within weeks of onset, before conservative care has had a fair trial (typically 6 to 12 weeks for non-red-flag cases).
- Skipping physiotherapy because it feels slow.
- Doctor-shopping for the most aggressive opinion rather than the most accurate one.
- Not seeking a second opinion when surgery is recommended. International guidelines and patient-advocacy bodies broadly support this.
How can I prevent a bulging disc from getting worse?
You can't reverse disc ageing, but you can reduce flare-ups and progression:
- Keep moving daily — walking counts.
- Build core and posterior chain strength gradually.
- Lift with hips and legs, not a rounded back.
- Manage body weight within a reasonable range.
- Stop smoking.
- Break up long sitting with brief movement every 30 to 45 minutes.
- Sleep enough; poor sleep amplifies pain perception.
There's no magic posture, mattress, or supplement. Consistency beats intensity.
When does the bulging disc vs herniated disc distinction actually matter?
The distinction matters most when surgery is being considered. A contained bulge rarely warrants surgery. A large extruded fragment compressing a nerve root with matching symptoms and failed conservative care is a different conversation. For day-to-day management — exercise, pain control, return to work — the label changes very little.
This is also where an independent second opinion can help. If a surgeon has recommended an operation, it's reasonable to ask: does the imaging finding match my symptoms? Have we exhausted non-surgical options appropriate for my case? What happens if I wait 6 more weeks?
FAQ
Is a bulging disc considered a herniated disc?
Not technically. A bulge is broad and contained; a herniation involves a focal tear with material pushing outward. The terms are often blurred in casual use.
Can a bulging or herniated disc heal on its own?
Yes. Many herniations shrink over months as the body reabsorbs the displaced material. Bulges typically remain but become asymptomatic.
Do I need an MRI for back pain?
Not initially. Most guidelines reserve MRI for symptoms lasting beyond 6 weeks, neurological signs, or red flags.
Will surgery cure my disc problem?
Surgery can relieve specific nerve-compression symptoms, particularly leg pain from a clear herniation. It is less reliable for back pain alone and is not a cure for disc ageing.
Should I get a second opinion before spine surgery?
Yes, in most cases this is reasonable and encouraged. Spine surgery is elective for the majority of disc conditions, and a second review can confirm or refine the plan.
Can I fly or travel with a herniated disc?
Usually yes, unless you have red-flag symptoms. Get up and walk every hour or so on long flights.
Conclusion
The honest answer to "bulging disc vs herniated disc — does it matter?" is: sometimes, but less than most patients fear. Both are common, both usually improve, and both are treated similarly in the first instance. What matters more is whether your symptoms match your imaging, whether red flags are present, and whether conservative care has been given a fair chance.
If you've been told you need spine surgery, take a breath. Ask whether the recommendation rests on imaging alone or on a clear correlation with your symptoms. Ask what happens if you wait. And consider an independent online second opinion before committing to an irreversible step. This article is educational and not a substitute for an in-person assessment by a clinician who knows your full history.
Spines are remarkably resilient. Most of the time, so are the people attached to them.